




Abstract
Background:To explore the optimal surgical approach for preschool children with obstructive sleep apnea (OSA) by comparing
changes in venous hematological parameters, Faces Pain Scale Revision (FPS-R) pain scale scores, and OSA-18 scale scores following
two different surgical treatments.
Methods: A total of 83 preschool children with OSA were enrolled, with 42 assigned to the control
group (total tonsillectomy with adenoidectomy) and 41 to the experimental group (partial tonsillectomy with adenoidectomy).
Preoperative and postoperative (3-day) measurements included cardiovascular disease risk factors, immune-related indicators,
perioperative blood loss, postoperative FPS-R pain scale scores, and OSA-18 scale scores. Data were analyzed using SPSS
29.0.20.
Results: Comparison between the two groups revealed no significant differences in intraoperative blood loss, primary
bleeding, pre- and post-treatment OSA-18 scale scores, C-reactive protein(CRP) levels, cardiovascular disease risk factors, or
immune-related indicators (all P > 0.05). However, significant differences were observed in secondary bleeding (P< 0.05) and
postoperative FPS-R pain scale grades (P< 0.05). In the control group, pre- and post-treatment antistreptolysin O(ASO) levels showed
no significant difference (P> 0.05), whereas in the experimental group, ASO levels decreased significantly (P< 0.05).
Conclusion:Partial tonsillectomy demonstrated comparable efficacy to total tonsillectomy in terms of intraoperative blood loss, reduction of
snoring symptoms, and improvement of airway patency, with both procedures achieving stable therapeutic outcomes. No significant
differences were observed between partial and total tonsillectomy regarding short-term effects on cardiovascular disease risk
factors or immune function. For preschool children with OSA, partial tonsillectomy was superior to total tonsillectomy in reducing
postoperative pain, secondary bleeding, and ASO levels.
Keywords:preschool OSA; immune function indicators; FPS-R pain scale.
Introduction
Childhood obstructive sleep apnea (OSA) refers to a series of pathophysiological changes caused by frequent partial or complete upper airway obstruction during children's sleep, interfering with children's normal ventilation and sleep structure. Currently, relevant literature reports that the prevalence of children is between 1.2% and 5.7%, and its peak incidence occurs between 2-8 years old, and increases with the rising trend of childhood obesity [1]. As early as 2016, foreign scholars pointed out that OSA can cause cognitive and neuropsychological dysfunction, Attention-Deficit Hyperactivity Disorder (ADHD), learning problems and nocturnal enuresis in children, and can even affect the development of the cardiovascular system and increase the prevalence of cardiovascular events such as hypertension in adults [2].
It can be said that OSA seriously affects children's physical development, and the anatomical causes are mainly physiological hypertrophy of adenoids and tonsils[1]. Currently, academia believes that respiratory obstruction of the upper airway in children with OSA can be well improved through tonsillectomy or adenoidectomy[3]. In the body's immune system, the tonsils (palatine tonsils) and adenoids (pharyngeal tonsils) are important parts of the pharyngeal lymph ring. They are located at the entrance of the upper airway and digestive tract, serving as the first line of defense against food and foreign microorganisms and other antigenic substances in the air, playing the dual role of cellular and humoral immunity[4]. Due to the increasing number of food types and increasing mobility among preschool children between the ages of 3-6, the digestive tract and respiratory tract of the body will receive various exogenous stimuli at this stage, but the body's immune system has not yet matured[5], and the tonsils, as the body's first line of defense of immunity, can produce a large number of immune factors at this stage, which helps to stimulate the body to gradually establish a natural resistance and immune ecological balance. However, there is still few relevant literature on the changes in immune function and vascular disease risk factors caused by different surgical methods in preschool children with OSA. Therefore, this study collected anti-streptolysin O, cardiovascular disease risk factors, immune function and other indicators after treatment in preschool children with OSA after two different surgical methods to provide some theoretical support for the choice of surgical methods in preschool children with OSA.
Methods
General informationA group of preschool children diagnosed with OSA from November 2022 to November 2023 from the Department of Otolaryngology Head and Neck Surgery of the Affiliated Hospital of Jiujiang University were selected. 90 patients met the "enrollment criteria" and were randomly divided into a control group (total tonsillectomy) and an experimental group (partial tonsillectomy) with 45 patients in each. Among them, 3 children in the control group and 4 children in the experimental group withdrew from the study due to their refusal to test relevant blood indicators and improve relevant scale evaluation after surgery.
Inclusion criteria:① The age of the child is between 3 and 6 years old. The Body Mass Index (BMI) value was less than 25, snoring ≥ 3 nights/week, and portable sleep monitoring: apnea-hypopnea index (AHI) ≥ 1. Rule out other underlying diseases. The parents of the child have basic education level and have clear language expression and thinking. ② According to the "Technical Standards for Standardized Treatment of Tonsil and Adenoid Low-Temperature Plasma Radiofrequency Ablation in Children" 3 for the grading of tonsil and adenoidal hypertrophy, the enrolled children met the requirements of degree III or IV of tonsil hypertrophy and degree III or IV of adenoidal hypertrophy. ③ No significant abnormalities were found in other routine preoperative examinations. The research content of this topic has been certified by the Ethics Committee of the Affiliated Hospital of Jiujiang University (approval number: NO. jjumer-b-2022-0612), and all parents of the children have signed the informed consent form.
MethodSurgical method: All enrolled children were transferred to the operating room before 9:00 AM on the day of surgery. During general anesthesia induction, anesthesiologists administered a single intravenous dose of fentanyl for analgesia.The children in the control group underwent total tonsillectomy with the capsule resected; the experimental group underwent partial tonsillectomy with the tonsillectomy preserved, the anterior and posterior arches preserved, and no mass tonsil tissue remained. All children underwent plasma ablation of hypertrophy of adenoids. The cutting instruments during the operation were plasma blades from Beijing Jesse Huizhong Technology Co.Ltd, and the operations were also completed by the same senior doctor.
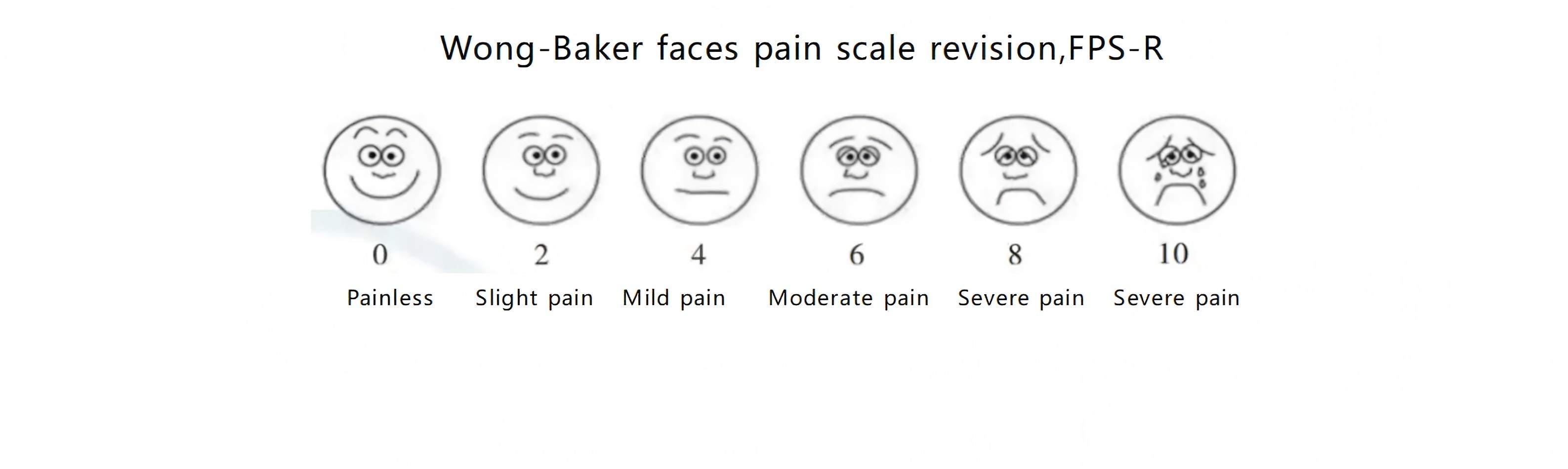
Observation indicators: Fasting venous blood was collected before and on the 3rd day after surgery to measure anti-streptolysin O, cardiovascular disease risk factors (serum total cholesterol, triglycerides, high-density lipoprotein cholesterol,low-density lipoprotein cholesterol, serum apolipoprotein A, serum apolipoprotein B, immune indicators (IgA, IgE, IgG, IgM, complement C3, complement C4), C-reactive protein (CRP), perioperative blood loss and postoperative OSA-18 scale scores of children in the two groups were counted This was because, considering the cognition and understanding level of children aged 3-6, we used Faces Pain Scale Revision (FPS-R) pain volume [3,6] to assess the pain of children one day after surgery (Figure 1).
Figure 1. FPS-R pain volume Pain levels assessed using the FPS-R scale pre- and post-operation.
All data were statistically analyzed using the statistical software SPSS29.0.20 system. The measurement data were expressed in Mean ± SD, the chi-square test was used, and the counting data were expressed in the number of cases. The contingency table analysis of non-parametric test was used. The comparison between the two groups before and after treatment was carried out using paired sample t-test. The comparison between the two groups was carried out using isolated sample t-test. The difference was P<0.05.
Results
Two sets of basic dataThe average age of the 42 children in the control group was 5.00±0.74 (years), the BMI was 18.14±3.52 (kg/m2), and the average course of disease was 10.00±4.75 (months); the average age of the 41 children in the experimental group was 4.87±0.85 (years), the BMI was 18.80±3.59, and the average course of disease was 10.46±4.65 (months). There were no statistically significant differences between the two groups in terms of total number of people, ratio of male to female, average age, BMI value, average course of disease, AHI, degree of tonsils and adenoids enlargement (P>0.05) ( Table 1).
Table 1. Comparison of two sets of basic data.
| Group | n | Gender | Average age(Y) | BMI(kg/m2) | Average course of disease (months) | AHI | Degree of tonsil enlargement | Adenoid enlargement degree | |||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Male | Female | III | IV | III | IV | ||||||
| Control Group | 42 | 28 | 14 | 5.00±0.74 | 18.14±3.52 | 10.00±4.75 | 5.56±2.46 | 32 | 10 | 33 | 9 |
| Experimental Group | 41 | 30 | 11 | 4.87±0.85 | 18.80±3.59 | 10.46±4.65 | 5.47±2.42 | 35 | 6 | 30 | 11 |
| F/t | -0.449 | 0.417 | 0.694 | -0.851 | -0.449 | 0.174 | 1.122 | 0.331 | |||
| P | 0.655 | 0.518 | 0.49 | 0.398 | 0.655 | 0.862 | 0.289 | 0.565 | |||
The treatment group showed a slightly higher mean volume (4.49 ± 1.05 mL) compared to the control group (4.43 ± 0.97 mL), with no significant difference (P = 0.790). For primary bleeding episodes, the control group had 4 cases versus 1 case in the treatment group, but this difference was not statistically significant (P = 0.371). In contrast, secondary bleeding events differed significantly between groups (9 cases in controls vs. 2 cases in treatment group, P = 0.026). This indicates that the treatment group had a statistically significant lower incidence of secondary bleeding compared to controls (Table 2).
Table 2. Perioperative bleeding profiles of the two groups.
| Group | n | Intraoperative Blood Loss(mL) | Primary Bleeding | Secondary Bleeding | ||
|---|---|---|---|---|---|---|
| Bleeding | No Bleeding | Bleeding | No Bleeding | |||
| Control Group | 42 | 4.43±0.97 | 4 | 38 | 9 | 33 |
| Experimental Group | 41 | 4.49±1.05 | 1 | 40 | 2 | 39 |
| F/t | -0.267 | 4.943 | ||||
| P | 0.79 | 0.026 | ||||
On postoperative day 1(Post-op Day 1), the control group showed mild pain:moderate pain = 15:27, while the treatment group demonstrated 34:7. On postoperative day 3(Post-op Day 3), the ratios were 10:32 (control) versus 26:15 (treatment). By postoperative day 10(Post-op Day 10), the distributions were 13:29 (control) and 23:18 (treatment). The treatment group exhibited significantly lower pain levels than the control group at all measured time points (postoperative days 1, 3, and 10), with all P-values <0.05, indicating statistically significant differences in pain experience between the two groups (Table 3).
Table 3. Postoperative pain levels according to FPS-R grading.
| Group | n | Post-op Day 1 | Post-op Day 3 | Post-op Day 10 | |||
|---|---|---|---|---|---|---|---|
| Mild Pain | Moderate Pain | Mild Pain | Moderate Pain | No Pain | Mild Pain | ||
| Control Group | 42 | 15 | 27 | 10 | 32 | 13 | 29 |
| Experimental Group | 41 | 34 | 7 | 26 | 15 | 23 | 18 |
| F/t | -0.449 | 19.123 | 13.25 | 5.341 | |||
| P | 0.655 | < 0.001 | < 0.001 | 0.021 | |||
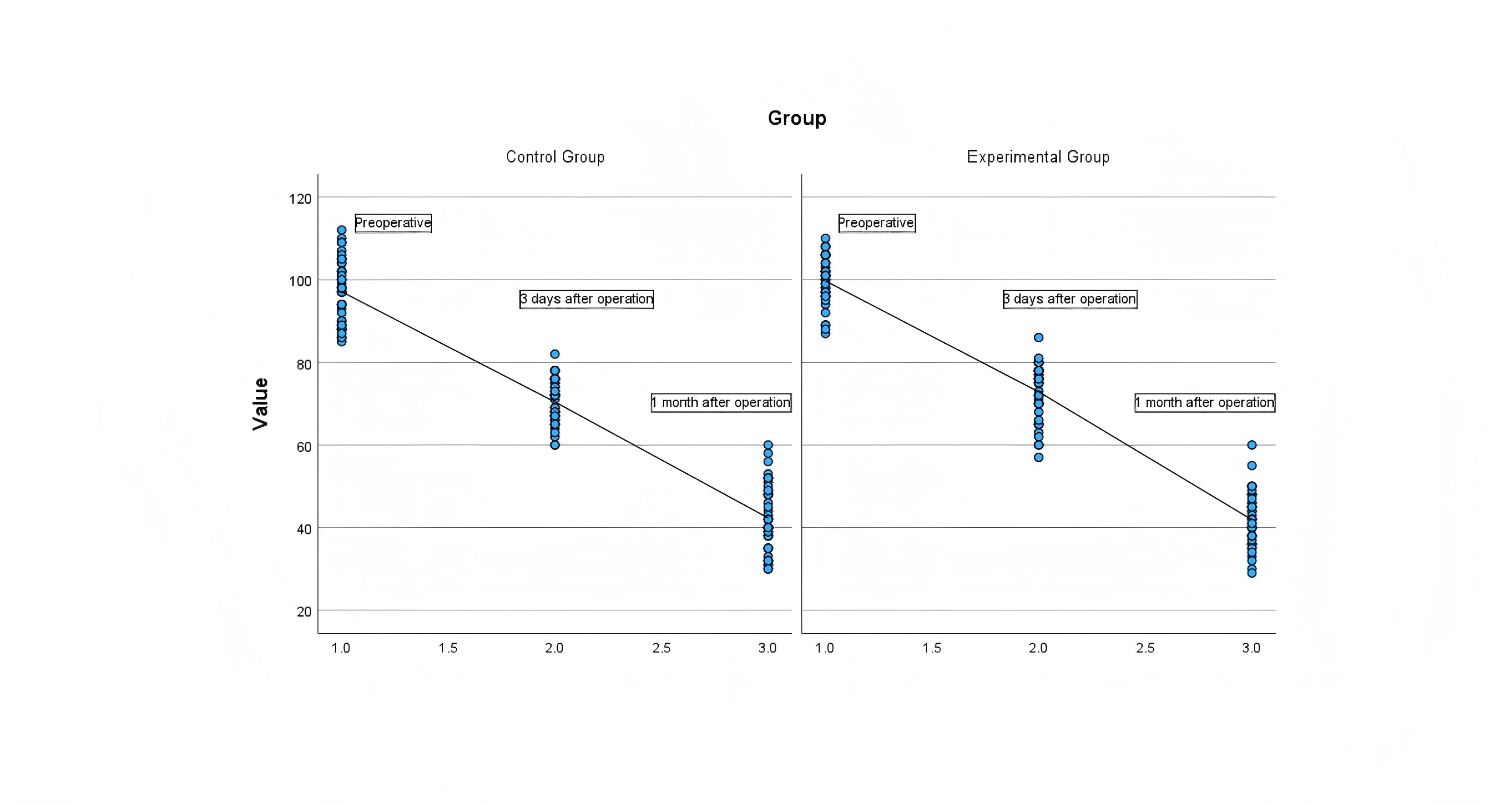
The scores of OSA-18 scale in the two groups before and after treatment. The OSA-18 scale scores of the two groups gradually decreased on preoperative,postoperative 3 days and postoperative1 month(Post-op Month 1) , but the P value compared between the two groups was greater than 0.05 (Figure 2), that is, there was no statistical difference in the OSA-18 scale scores between the two groups at each stage before and after treatment (Table 4).
Table 4. Preoperative and Postoperative OSA-18 Scale Evaluations.
| Group | n | Pre-op | Post-op Day 3 | Post-op Month 1 |
|---|---|---|---|---|
| Control Group | 42 | 97.07±7.71 | 70.40±5.28 | 42.33±8.14 |
| Experimental Group | 41 | 99.68±5.74 | 72.73±6.72 | 41.90±6.69 |
| T | -0.449 | -1.753 | -1.848 | 0.263 |
| P | 0.655 | 0.084 | 0.068 | 0.793 |
Figure 2. Scatterplot of OSA-18 scale scores in the two groups before and after treatment Treatment efficacy was assessed by comparing OSA-18 scores between the two groups at preoperative, postoperative day 3, and postoperative month 1 time points, with P < 0.05 considered statistically significant.
The mean value of ASO in both groups decreased before and after treatment. The P value in the control group was greater than 0.05, and the P value in the experimental group was 0.019(<0.05), which was statistically significant (Table 5).
Table 5. ASO indicators before and after treatment in the two groups.
| Test | Group | Pre-op | Post-op Day 3 | T | P |
|---|---|---|---|---|---|
| ASO (IU/mL) | Control Group | 184.67±236.71 | 179.57±237.10 | 1.905 | 0.064 |
| Experimental Group | 94.94±116.82 | 89.11±110.25 | 2.441 | 0.019 |
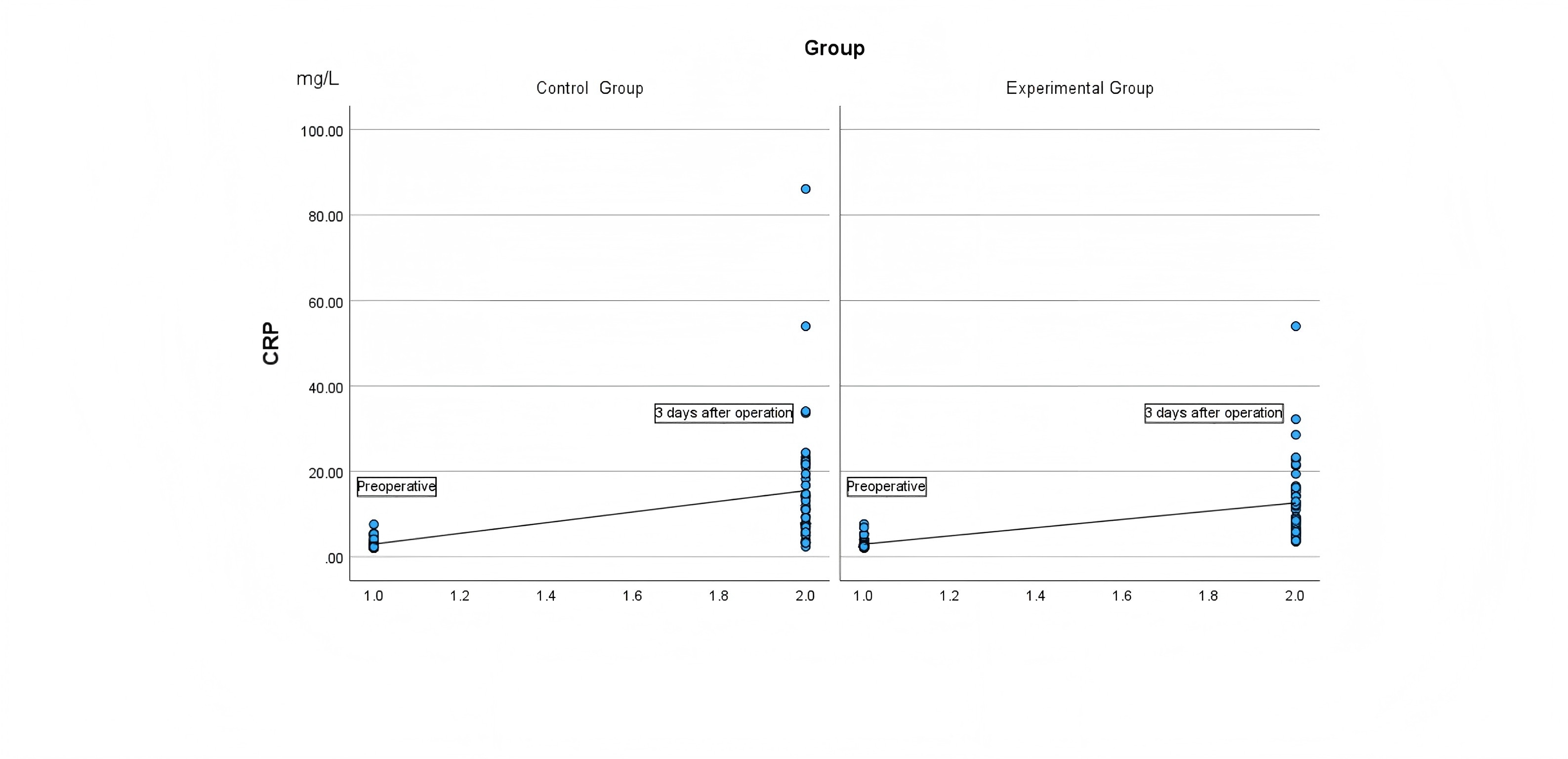
The mean value of CRP in both groups increased before and after treatment and the P values were greater than 0.05 before and after treatment, which was not statistically significant (Figure 3, Table 6).
Table 6. CRP indicators before and after treatment in both groups.
| Test | Time | Control Group | Experimental Group | T | P |
|---|---|---|---|---|---|
| CRP (mg/L) | Pre-op | 2.98±1.26 | 2.97±1.24 | 0.047 | 0.963 |
| Post-op Day 3 | 15.48±15.11 | 12.62±9.67 | 1.027 | 0.307 |
Figure 3.Scatter plots of CRP values in the two groups before and after treatment Inflammation status was assessed by comparing CRP values between the two groups at preoperative and postoperative day 3 time points, with P < 0.05 considered statistically significant.
The mean values of total cholesterol, triglyceride, low-density lipoprotein, and apolipoprotein B indicators in the two groups showed an upward trend before and after treatment , and the P values were all greater than 0.05. There was no statistical difference between the two groups before and after treatment; The mean values of high-density lipoprotein and apolipoprotein A1 in the two groups showed a downward trend before and after treatment, and the P values were all greater than 0.05. There was no statistical difference between the two groups before and after treatment (Table 7).
Table 7. Cardiovascular disease risk factor indicators before and after treatment in group.
| Test | Time | Control Group | Experimental Group | T | P |
|---|---|---|---|---|---|
| TC (mmol/L) | Pre-op | 4.13±0.64 | 4.33±0.83 | -1.21 | 0.23 |
| Post-op Day 3 | 4.42±0.74 | 4.62±0.97 | -1.08 | 0.284 | |
| TG (mmol/L) | Pre-op | 0.854±0.35 | 0.98±0.43 | -1.421 | 0.159 |
| Post-op Day 3 | 1.14±0.32 | 1.19±0.35 | -0.726 | 0.47 | |
| HDL (mmol/L) | Pre-op | 1.55±0.26 | 1.57±0.25 | -0.328 | 0.744 |
| Post-op Day 3 | 1.47±0.25 | 1.49±0.20 | -0.327 | 0.744 | |
| LDL (mmol/L) | Pre-op | 2.30±0.43 | 2.46±0.56 | -1.454 | 0.15 |
| Post-op Day 3 | 2.53±0.48 | 2.66±0.66 | -1.033 | 0.304 | |
| Apo-A1 (g/L) | Pre-op | 1.37±0.18 | 1.36±0.16 | 0.064 | 0.949 |
| Post-op Day 3 | 1.32±0.18 | 1.31±0.15 | 0.422 | 0.674 | |
| Apo-B (g/L) | Pre-op | 0.87±0.21 | 0.93±0.30 | -0.97 | 0.335 |
| Post-op Day 3 | 1.06±0.22 | 1.15±0.36 | -1.342 | 0.183 |
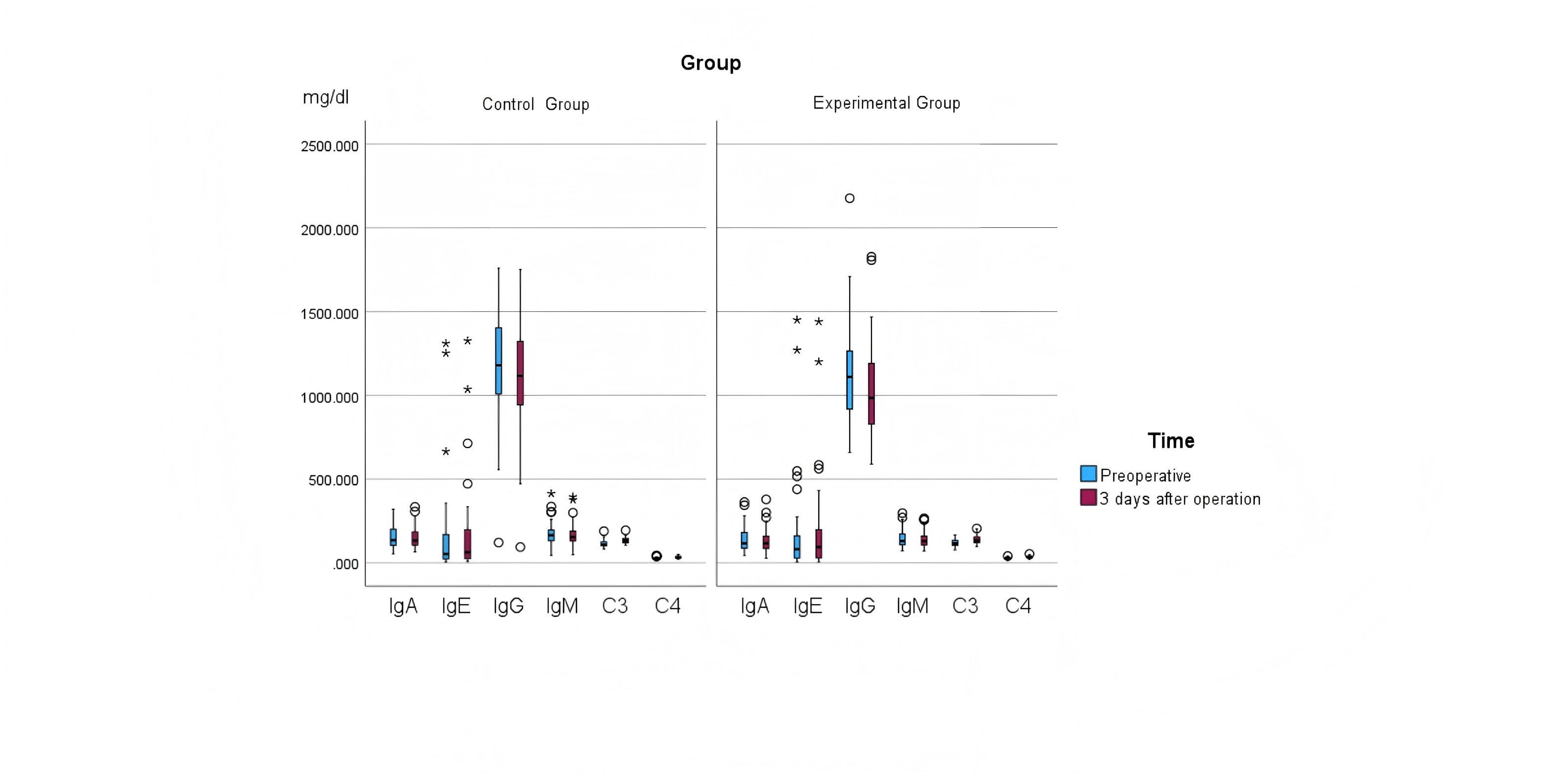
The mean values of IgA and IgG in both groups decreased before and after treatment, with P values greater than 0.05, that is, there was no statistical significance between IgA and IgG before and after treatment. The mean value of IgE in both groups increased after treatment, and the P value was greater than 0.05, that is, there was no statistical significance between the two groups before and after treatment in IgE. The mean values in both groups decreased after IgM immunization treatment, and the P values were less than 0.05, that is, the differences between the two groups before and after treatment were statistically significant (Figure 4). The mean values of complement C3 and complement C4 in both groups increased before and after treatment, and the P values were greater than 0.05, that is, there was no statistical significance between the two groups before and after treatment (Table 8).
Table 8. Immunity-related indicators before and after treatment in the two groups.
| Test | Time | Control Group | Experimental Group | T | P |
|---|---|---|---|---|---|
| IgA (mg/dL) | Pre-op | 152.73±68.85 | 139.51±75.19 | 0.836 | 0.406 |
| Post-op Day 3 | 152.93±66.56 | 134.84±72.22 | 1.187 | 0.239 | |
| IgE (mg/dL) | Pre-op | 159.31±283.16 | 179.53±300.44 | -0.315 | 0.753 |
| Post-op Day 3 | 166.31±271.34 | 191.12±294.10 | -0.4 | 0.69 | |
| IgG (mg/dL) | Pre-op | 1187.02±351.16 | 1108.05±293.43 | 1.11 | 0.27 |
| Post-op Day 3 | 1126.57±335.46 | 1031.62±286.88 | 1.384 | 0.17 | |
| IgM (mg/dL) | Pre-op | 173.75±72.82 | 144.59±53.00 | 2.082 | 0.041 |
| Post-op Day 3 | 170.77±70.58 | 139.01±48.65 | 2.382 | 0.02 | |
| C3 (mg/dL) | Pre-op | 115.68±21.68 | 117.90±20.03 | -0.484 | 0.629 |
| Post-op Day 3 | 134.06±18.38 | 137.52±24.70 | -0.727 | 0.469 | |
| C4 (mg/dL) | Pre-op | 26.71±6.23 | 27.55±5.89 | -0.627 | 0.532 |
| Post-op Day 3 | 33.57±7.33 | 34.34±6.54 | -0.507 | 0.614 |
Figure 4. Box plots of immune-related indicators before and after treatment in the two groups Treatment efficacy was evaluated by comparing serological immune markers (IgA, IgE, IgG, IgM, C3, and C4) between the two groups at preoperative and postoperative day 3 time points, with P < 0.05 considered statistically significant.
Discussion
Research on the impact of tonsillectomy on immune function in children has long become a hot topic of clinical research in the academic community. Wang Xianghui and other scholars reported many years ago that after tonsillectomy in children, the incidence of chronic inflammation in the upper respiratory tract will increase, and symptoms such as foreign body sensation and dry throat discomfort will be prone to occur in adulthood[7]. It is recommended that for children without obvious inflammation of the tonsils, while surgically resolving the obstruction, some of the functions of the tonsils should be preserved as much as possible. In a 10-year follow-up study, Eviatar[8] confirmed that there was no significant difference in snoring, airway patency, daily diet and upper airway inflammation between children undergoing partial tonsillectomy and children undergoing total tonsillectomy, and stable results could be achieved.
The ages of 3 to 6 are preschool. During this period, children's height and weight continue to increase, their exercise ability continues to increase, and their curiosity about surrounding things and their ability to learn are also very strong. Therefore, this stage is a key stage for children's development stage.OSA is also a peak in preschool age. It will not only affect children's sleep quality, growth and development speed and the production of "adenoid features", but long-term hypoxia will also lead to activation of the nervous system and disorders of the endocrine system increase the probability of cardiovascular diseases, ADHD and emotional disorders in children[9]. With the rapid development of information transmission media, parents understand the importance of early intervention and early treatment of children with OSA. However, which surgical method is safer and has better results has always been a concern for parents.
This study used relevant literature as a reference, and used the indicators of total cholesterol, triglycerides, high-density lipoprotein cholesterol, low-density lipoprotein cholesterol, serum apolipoprotein A1, and serum apolipoprotein B in serum blood test as entry points to study the risk-related factors of cardiovascular disease[10], and used IgA, IgE, IgG, IgM, complement C3 and complement C4 as entry points to study the indicators related to humoral immune function of the body[11]. The results of this study showed that there were no statistically significant differences in intraoperative blood loss and changes in OSA-18 scale scores before and after surgery between the control group and the experimental group. Three days after partial or total tonsillectomy, the mean values of total cholesterol, triglycerides, low-density lipoprotein, and apolipoprotein B showed an increasing trend, while the mean values of high-density lipoprotein and apolipoprotein A1 showed a decreasing trend, but they were all within the normal range, and there was no statistical significance between the two groups. Postoperative cardiovascular disease risk-related indicators in both groups of children tended to increase the possibility of cardiovascular disease. This may be related to the impact of preoperative fasting and general anesthesia on liver metabolic function in children, and may also be related to the stress response caused by surgical procedures on the body. Thinking further, this result coincidentally proves that for people with poor control such as coronary heart disease, hyperlipidemia and hypertension, the possibility of worsening cardiovascular and cerebrovascular diseases needs to be specifically explained before undergoing general anesthesia surgery.
In this study, IgA, IgG, and IgM showed a downward trend before and after treatment. This shows that no matter which kind of surgery is performed, the humoral immune function of children will decline in the short term after surgery, but within the normal range, which is consistent with the research results of Chengyong Zhou and other scholars [12]. In addition, the mean values of IgE, complement C3, complement C4, and CRP increased in both groups, and there was no statistically significant difference between the two groups. Serum IgE is generally related to age. The normal value in children is generally higher than that in adults. Its increase is mainly related to allergic diseases and immune system diseases; the increase of complement C3, complement C4, and CRP may all be related to the production of acute inflammation. Therefore, it is speculated that the increase in IgE, complement C3, complement C4, and CRP values after surgery may be related to the resection of tonsils and adenoids, the weakening of the body's immune defenses, and the inflammatory state of the body triggered by the trauma caused by the surgical operation.
There were no statistically significant differences in intraoperative blood loss and changes in OSA-18 scale scores before and after surgery between the control group and the experimental group in this study. This shows that there is no significant difference between partial tonsillectomy and total tonsillectomy in terms of intraoperative blood loss, postoperative improvement of airway patency, and reduction of nocturnal hypoxemia, and stable curative effects can be achieved. In this study, the ASO of both groups of children showed a downward trend after surgery, and the decrease in ASO in the partial tonsillectomy group was even more obvious. That is, for preschool children, partial tonsillectomy may be more beneficial to reducing ASO than total tonsillectomy. On the other hand, this may happen to verify the results of Shuai Wang et al.'s study [13]-partial tonsillectomy is more suitable for children of all ages with a history of repeated respiratory infections, and can reduce the impact on immune function., and reduce the rate of postoperative respiratory infection.
The postoperative FPS-R pain scale scores demonstrated significantly lower pain perception in children undergoing partial tonsillectomy compared to total tonsillectomy (P<0.01). This reduction may be attributed to preservation of the tonsillar capsule during partial tonsillectomy, which minimizes exposure of submucosal vasculature and the pharyngeal constrictor muscles. Regarding postoperative hemorrhage, both primary bleeding (within 24 hours) and secondary bleeding (>24 hours) manifested only as blood-tinged sputum in all cases, which resolved spontaneously with ice-water gargles. Statistical analysis revealed significantly lower secondary bleeding rates in the partial tonsillectomy group (4.9% vs 21.4%, P=0.026), consistent with Qiu et al.'s findings demonstrating reduced bleeding risks with this technique[14]. We hypothesize that partial tonsillectomy's dual advantages – avoiding muscle exposure and reducing pain-related fluid/food avoidance – promote earlier nutritional recovery and wound healing, thereby decreasing secondary bleeding risks
Conclusion
Partial tonsillectomy achieves comparable outcomes to total tonsillectomy in improving airway obstruction, cardiovascular parameters, and immune function, while offering superior benefits in reducing ASO levels (P=0.019), postoperative pain (P<0.005), and secondary bleeding rates (P=0.026). For preschool OSA patients without chronic tonsillitis history, we recommend partial tonsillectomy when tonsillar hypertrophy is the primary etiology. This approach optimizes long-term health outcomes and alleviates parental concerns regarding postoperative complications.
Abbreviations
Apo-A1: Apolipoprotein A; Apo-B: Apolipoprotein B; ADHD: Attention-Deficit Hyperactivity Disorder; AHI: Apnea-hypopnea index; ASO: Antistreptolysin O; CRP: C-reactive protein; C3: Complement C3; C4: Complement C4; FPS-R: Faces Pain Scale Revision; HDL: High-density lipoprotein cholesterol; LDL: Low-density lipoprotein cholesterol; IgA: Immunoglobulin A; IgE: Immunoglobulin E; IgG: Immunoglobulin G; IgM: Immunoglobulin M; OSA: Obstructive Sleep Apnea; BMI: The Body Mass Index; TC: Total Cholesterol; TG: Triglycerides;
Declarations
Author Contributions
The specific contributions to this study are as follows: Yuan Jinjin: Conceptualization, Methodology, Data curation, Writing – Original Draft. Wei Yonghao: Surgical technical support, Writing – Review & Editing. Yi Jianqi: Provision of critical study materials, Formal analysis, Discussion of results. Liu Yaling: Data curation, Validation. Fei Hongxia: Data curation, Validation. All authors have reviewed and approved the final manuscript for submission. Wei Yonghao (Corresponding Author) oversaw the overall coordination of the manuscript, finalized the draft, and managed submission-related matters.
Acknowledgements
We sincerely thank Doctor Wei Yonghao for his guidance on this research project and his assistance in data collection. We are also grateful to Yi Jianqi, Liu Yaling, and Fei Hongxia for their contributions to data gathering. Our special thanks go to the Affiliated Hospital of Jiujiang University for their support of this study.
Funding information
Jiangxi Provincial Health Commission Science and Technology Program Number: 202311512
Ethics Approval and Consent to Participate
This study was reviewed and approved by the Ethics Committee of Jiujiang University Affiliated Hospital (Approval No. jjumer-b-2022-0612). All research procedures involving human participants were conducted in accordance with the principles outlined in the Declaration of Helsinki and its subsequent amendments. Written informed consent was obtained from all participants.
Competing Interests
The authors declare that they have no existing or potential commercial or financial relationships that could create a conflict of interest at the time of conducting this study.
Data availability
Not Applicable.
References
 Figures
Figures References
References Peer
Peer Information
InformationFigure 1. FPS-R pain volume Pain levels assessed using the FPS-R scale pre- and post-operation.
Figure 2. Scatterplot of OSA-18 scale scores in the two groups before and after treatment Treatment efficacy was assessed by comparing OSA-18 scores between the two groups at preoperative, postoperative day 3, and postoperative month 1 time points, with P < 0.05 considered statistically significant.
Figure 3.Scatter plots of CRP values in the two groups before and after treatment Inflammation status was assessed by comparing CRP values between the two groups at preoperative and postoperative day 3 time points, with P < 0.05 considered statistically significant.
Figure 4. Box plots of immune-related indicators before and after treatment in the two groups Treatment efficacy was evaluated by comparing serological immune markers (IgA, IgE, IgG, IgM, C3, and C4) between the two groups at preoperative and postoperative day 3 time points, with P < 0.05 considered statistically significant.
Peer-review Terminology
Identity transparency: Single anonymized
Reviewer interacts with: Editor
Details
This is an open access article under the terms of the Creative Commons Attribution License(http://creativecommons.org/licenses/by/4.0/), which permits use, distribution and reproduction in any medium, provided the original work is properly cited.
Publication History
Received 2025-06-07
Accepted 2025-07-18
Published 2025-08-10