




Abstract
Objective: To investigate the etiology of difficult decannulation in patients with long-term tracheostomy following brain-related diseases, and to explore the preoperative examination and assessment, selection of surgical indications, surgical and postoperative management methods. This aims to provide a scientific basis for facilitating successful decannulation, improving patients' quality of life, and guiding clinical practitioners in the management of such cases.
Methods: A retrospective analysis was conducted on 27 patients who were hospitalized in our department from May to December 2025 and had experienced failed decannulation after long-term tracheostomy. Preoperative examination and assessment included electronic laryngoscopy and laryngotracheal CT three-dimensional reconstruction. Electronic laryngoscopy was simultaneously used to assess swallowing function, including the Penetration-Aspiration Scale score, Murray Secretion Scale score, vallecula and pyriform sinus residue grading, and swallowing disability grading and classification. The surgical procedure involved endoscopic-assisted resection of laryngeal and tracheal granulation tissue via a supporting laryngoscope under general anesthesia.
Results: The primary cause of laryngotracheal stenosis leading to decannulation failure in patients with long-term tracheostomy due to brain diseases was obstruction from granulation tissue hyperplasia within the larynx and trachea, followed by restricted bilateral vocal cord abduction. Based on detailed preoperative examinations and assessments, all 27 patients in this group were deemed suitable candidates for surgery. They successfully underwent endoscopic-assisted resection of laryngeal and tracheal granulation tissue via a supporting laryngoscope under general anesthesia without any complications. Decannulation was successfully achieved in all patients within 7 to 10 days postoperatively.
Conclusions: 1) Electronic fiberoptic laryngoscopy and laryngotracheal CT three-dimensional reconstruction are effective methods for preoperative examination and evaluation. 2) Appropriate surgical candidates can be selected based on these two examinations. 3) Endoscopic-assisted resection of laryngotracheal granulation lesions via a supporting laryngoscope under general anesthesia is a safe and effective method to resolve decannulation difficulties in such patients.
Keywords: Brain diseases; Tracheotomy; Laryngotracheal stenosis; Difficult decannulation.
Introduction
Brain-related diseases such as cerebral hemorrhage, brain tumor postoperative states, and traumatic brain injury often lead to weakened respiratory function or difficulty breathing, necessitating tracheotomy. Since these brain conditions frequently result in prolonged coma or impaired consciousness, treatment and rehabilitation periods are extended, requiring long-term cannulation to maintain airway patency. When patients' brain conditions stabilize and they enter the rehabilitation phase, long-term cannulation inevitably poses significant challenges to recovery and nursing care, severely impacting the quality of life for both patients and their families. Decannulation becomes essential. However, due to prolonged cannulation, some patients cannot undergo decannulation smoothly. This article aims to investigate the causes of decannulation difficulties, preoperative examination and assessment, selection of surgical indications, and surgical and postoperative management strategies for patients with long-term tracheostomy cannulation following brain-related diseases, through a retrospective analysis of 27 cases admitted to our department between May and December 2025. The goal is to facilitate successful decannulation, improve patients' quality of life, and provide scientific evidence for clinicians managing such cases.
Materials and Methods
Patients
From May to December 2025, our department treated 27 patients who failed decannulation after tracheotomy due to brain-related diseases. Among them, 18 were male and 9 were female, aged ranging from 17 to 84 years, with a mean age of 47.52 ± 17.20 years. In our study cohort, obstructions were primarily localized at the previous tracheostomy stoma site. The duration of cannulation ranged from 1 to 15 months, with a mean duration of 5.19 ± 4.08 months. The primary brain diseases included cerebral hemorrhage (16 cases), brain tumor (2 cases), cerebral infarction (1 case), and severe traumatic brain injury (8 cases), as shown in Table 1.
Table 1. Baseline Characteristics of Patients with Laryngotracheal Stenosis.
| Baseline Data | Sex | Age | Mean Age (x̄±s) | Primary Disease | Tube indwelling time (month) | Average Tube Indwelling Time (x̄±s) |
|---|---|---|---|---|---|---|
| Zeng** | male | 51 | 47.52 ± 17.20 | Cerebral Artery Stenosis | 3 | 5.19 ± 4.08 |
| Tang* | male | 45 | Brainstem Hemorrhage | 12 | ||
| Li** | female | 51 | Brainstem Hemorrhage | 3 | ||
| Lai** | male | 26 | Intracerebral Hemorrhage | 2 | ||
| Lin** | male | 71 | Intracerebral Hemorrhage | 3 | ||
| Xie** | male | 61 | Cerebral Infarction | 3 | ||
| Yu** | male | 37 | Traumatic Brain Injury | 2 | ||
| Huang** | male | 27 | Intracerebral Hemorrhage | 5 | ||
| Chen** | female | 61 | Intracerebral Hemorrhage | 3 | ||
| Jing** | female | 55 | Intracerebral Hemorrhage | 3 | ||
| Chen** | female | 17 | Brainstem tumor | 10 | ||
| Lai** | male | 69 | Intracerebral Hemorrhage | 2 | ||
| Ye** | male | 62 | Intracerebral Hemorrhage | 2 | ||
| Zhang** | male | 43 | Intracerebral Hemorrhage | 5 | ||
| Zeng** | female | 58 | Traumatic Brain Injury | 11 | ||
| Xie* | male | 65 | Traumatic Brain Injury | 11 | ||
| Hu** | female | 19 | Intracerebral Hemorrhage | 1 | ||
| Liu** | male | 19 | Traumatic Brain Injury | 5 | ||
| Feng** | male | 46 | Intracerebral Hemorrhage | 10 | ||
| Luo** | female | 43 | Intracerebral Hemorrhage | 5 | ||
| Wu** | male | 56 | Traumatic Brain Injury | 3 | ||
| Su** | male | 44 | Traumatic Brain Injury | 1 | ||
| Ran** | male | 42 | Intracerebral Hemorrhage | 1 | ||
| Li* | male | 37 | Brainstem Hemorrhage | 8 | ||
| Deng** | female | 32 | Traumatic Brain Injury | 10 | ||
| Lu** | female | 84 | Intracerebral Hemorrhage | 1 | ||
| Kang** | male | 62 | postoperative brain tumor | 15 |
Decannulation
We defined successful extubation as the lack of need for reintubation within 24 hours of successful tracheostomy tube withdrawal.
Occlusion protocol: The patient needs to switch to an airless catheter (or with the airbag completely deflated) and undergo a 24-hour full occlusion test throughout the day.
Objective respiratory indicators: During the occlusion period, the patient must maintain a resting blood oxygen saturation (SpO2) of >90% without oxygen inhalation, and there should be no symptoms such as breathing difficulty, wheezing, or excessive sweating.
Failure criteria: If the patient experiences a sustained SpO2 below 90% after occlusion or tube removal, develops respiratory distress, severe wheezing sounds, requires reopening of the airway, or reinsertion of the tracheal tube, it is considered a failed tube removal.
Long-term tracheostomy: tube dependency for over 30 days.
Surgical Intervention
All surgical interventions were performed under general anesthesia. The airway lesions were exposed utilizing a suspension laryngoscope. Granulation tissue excision was performed using low-temperature plasma coblation, and precise hemostasis was achieved intraoperatively via plasma radiofrequency ablation. Regarding the ventilation strategy, standard positive pressure ventilation was maintained through the pre-existing tracheostomy tube or via an endotracheal tube placed directly through the stoma, without the need for high-frequency jet ventilation.
For the postoperative decannulation pathway, routine endoscopic re-evaluation was not performed. Instead, decannulation decisions were guided by a strict clinical protocol. Once postoperative reactive edema was clinically determined to have subsided (typically 2 days post-surgery), patients underwent a continuous capping trial. Successful decannulation was strictly based on objective clinical criteria (stable SpO2 >90%, and absence of stridor or distress during the occlusion trial), rather than anatomic visualization via post-operative endoscopy.
Fiberoptic Endoscopic Evaluation of Swallowing (FEES)
Evaluation Method: Fiberoptic Endoscopic Evaluation of Swallowing (FEES) was performed for all participants in this study.
Test Boluses and Procedure: Three bolus consistencies were utilized during the assessment: low-viscosity (thin liquid), medium-viscosity (thick liquid), and high-viscosity (paste). All boluses were tinted with green additives (e.g., natural spinach juice) to enhance visualization and contrast during the endoscopic procedure.
Preoperative Examination and Assessment
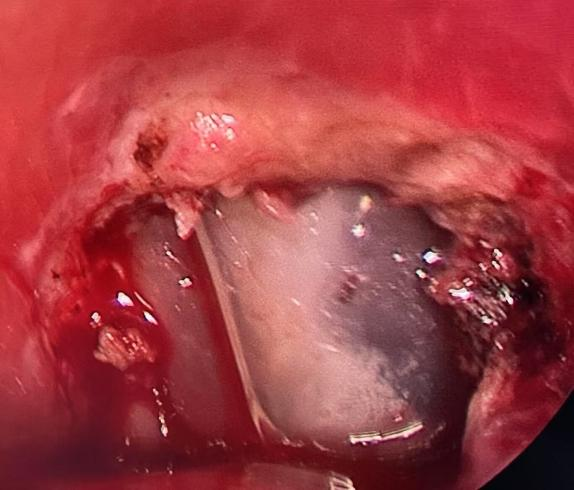
The results of electronic laryngoscopy and swallowing function assessment are presented in Table 2. Three-dimensional reconstruction images of the laryngotracheal CT are shown in Figure 1. Preoperative and postoperative images of laryngoscopy are shown in Figure 2 and Figure 3.
Table 2. Electronic Laryngoscopy Assessment Form for Patients with Laryngotracheal Stenosis.
| Baseline Data | Swallowing Impairment Score (Residue Rating) — Adduction | Swallowing Impairment Score (Residue Rating) — Abduction | Swallowing Impairment Score (Residue Rating) | Penetration-Aspiration Scale (PAS) | Percentage of Airway Occlusion (%) |
|---|---|---|---|---|---|
| Zeng** | left: normal right: normal |
left: normal right: normal |
Dysphagia (not have) valleculae: Trace Pyriform Sinus: Trace |
1 | 80 |
| Tang** | left: reduce right: reduce |
left: normal right: normal |
Dysphagia (Oropharyngeal Phase) valleculae: Mild Pyriform Sinus: Mild |
5 | 70 |
| Li** | left: reduce right: reduce |
left: reduce right: reduce |
Dysphagia (Oropharyngeal Phase) valleculae: Trace Pyriform Sinus: Mild |
5 | 80 |
| Lai** | left: normal right: normal |
left: normal right: normal |
Dysphagia (Oropharyngeal Phase) valleculae: Trace Pyriform Sinus: Trace |
4 | 100 |
| Lin** | left: normal right: fixed |
left: normal right: fixed |
Dysphagia (Oropharyngeal Phase) valleculae: Mild Pyriform Sinus: Trace |
6 | 70 |
| Xie** | left: reduce right: reduce |
left: reduce right: reduce |
Dysphagia (Oropharyngeal Phase) valleculae: Mild Pyriform Sinus: Moderate |
4 | 50 |
| Yu** | left: reduce right: reduce |
left: reduce right: reduce |
Dysphagia (Oropharyngeal Phase) valleculae: Moderate Pyriform Sinus: Moderate |
4 | 100 |
| Huang** | left: reduce right: normal |
left: reduce right: normal |
Dysphagia (Oropharyngeal Phase) valleculae: Moderate Pyriform Sinus: Moderate |
6 | 90 |
| Chen** | left: reduce right: reduce |
left: reduce right: reduce |
Dysphagia (Oropharyngeal Phase) valleculae: Trace Pyriform Sinus: Trace |
5 | 90 |
| Jing** | left: reduce right: reduce |
left: reduce right: reduce |
Dysphagia (Oropharyngeal Phase) valleculae: Mild Pyriform Sinus: Mild |
4 | 80 |
| Chen** | left: reduce right: reduce |
left: reduce right: reduce |
Dysphagia (Oropharyngeal Phase) valleculae: Mild Pyriform Sinus: Moderate |
4 | 95 |
| Lai** | left: fixed right: reduce |
left: fixed right: reduce |
Dysphagia (Not assessed) valleculae: Mild Pyriform Sinus: Mild |
/ | 60 |
| Ye** | left: fixed right: normal |
left: fixed right: normal |
Dysphagia (Oropharyngeal Phase) valleculae: Mild Pyriform Sinus: Mild |
4 | 60 |
| Zhang** | left: reduce right: reduce |
left: reduce right: reduce |
Dysphagia (Oropharyngeal Phase) valleculae: Mild Pyriform Sinus: Mild |
2 | 50–55 |
| Zeng** | left: reduce right: reduce |
left: normal right: normal |
Dysphagia (Oropharyngeal Phase) valleculae: Mild Pyriform Sinus: Mild |
5 | 98 |
| Xie** | left: reduce right: reduce |
left: normal right: normal |
Dysphagia (Oropharyngeal Phase) valleculae: Mild Pyriform Sinus: Mild |
5 | 50 |
| Hu** | left: reduce right: reduce |
left: normal right: normal |
Dysphagia (Oropharyngeal Phase) valleculae: Mild Pyriform Sinus: Mild |
4 | 70 |
| Liu** | left: reduce right: reduce |
left: normal right: normal |
Dysphagia (Oropharyngeal Phase) valleculae: Mild Pyriform Sinus: Mild |
5 | 40 |
| Feng** | left: reduce right: reduce |
left: normal right: normal |
Dysphagia (Oropharyngeal Phase) valleculae: Severe Pyriform Sinus: Severe |
7 | 70–75 |
| Luo** | left: normal right: normal |
left: normal right: normal |
Dysphagia (Oropharyngeal Phase) valleculae: Moderate Pyriform Sinus: Moderate |
4 | 55–60 |
| Wu** | left: reduce right: reduce |
left: reduce right: reduce |
Dysphagia (Oropharyngeal Phase) valleculae: Moderate Pyriform Sinus: Moderate |
6 | 100 |
| Su** | left: normal right: normal |
left: normal right: normal |
Dysphagia (Oropharyngeal Phase) valleculae: Mild Pyriform Sinus: Mild |
4 | 40 |
| Ran** | left: reduce right: reduce |
left: normal right: normal |
Dysphagia (Oropharyngeal Phase) valleculae: Mild Pyriform Sinus: Mild |
4 | / |
| Li* | left: reduce right: reduce |
left: normal right: normal |
Dysphagia (Oropharyngeal Phase) valleculae: Moderate Pyriform Sinus: Moderate |
6 | 60–65 |
| Deng** | left: reduce right: reduce |
left: normal right: normal |
Dysphagia (Oropharyngeal Phase) valleculae: Mild Pyriform Sinus: Mild |
5 | 100 |
| Lu** | left: reduce right: reduce |
left: normal right: normal |
Dysphagia (Oropharyngeal Phase) valleculae: Mild Pyriform Sinus: Mild |
4 | 90 |
| Kang** | left: reduce right: reduce |
Unable to abduct, fixed in the paramedian position | Dysphagia (Oropharyngeal Phase) valleculae: Mild Pyriform Sinus: Mild |
3 | / |
Figure 1. Laryngotracheal CT Image.
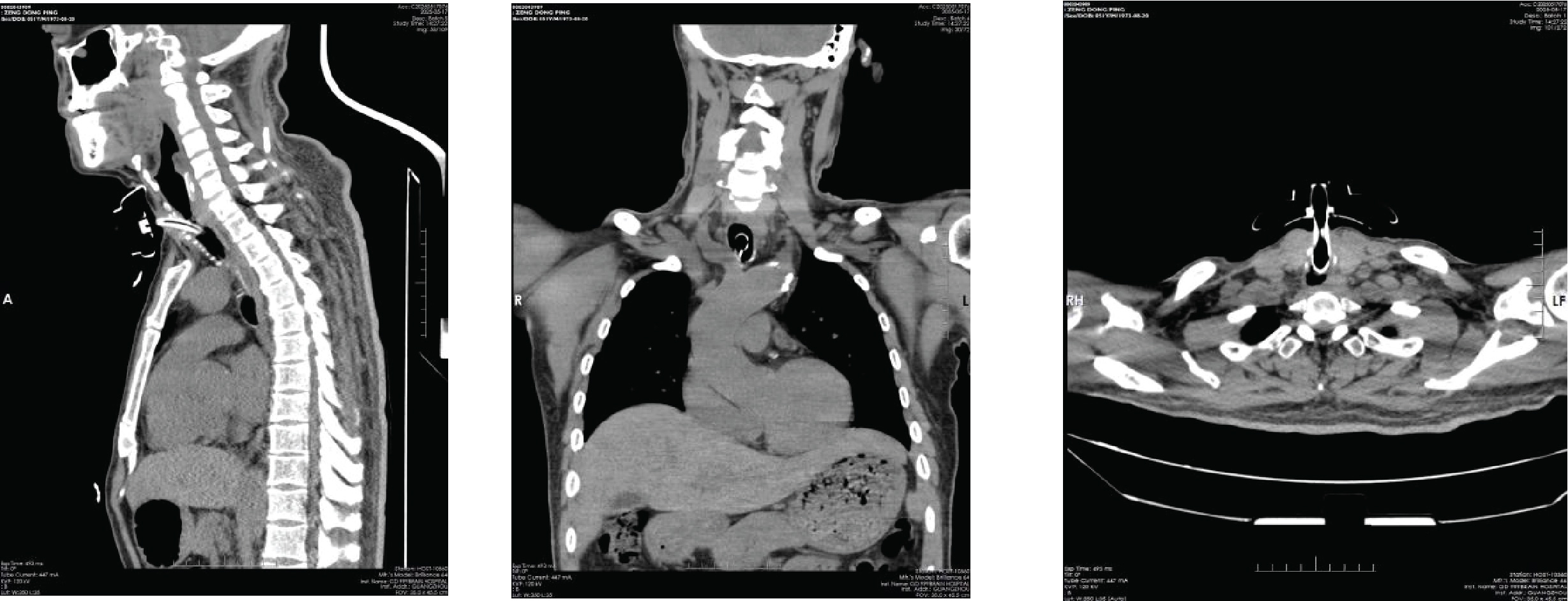
Figure 2. Preoperative images of laryngoscopy.
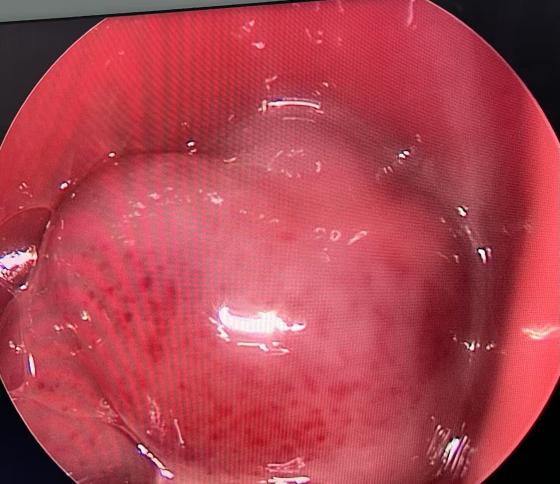
Figure 3. Postoperative images of laryngoscopy.
Surgical Indication Selection
Patients with long-term tracheostomy tube dependence after tracheotomy, whose primary disease does not cause dyspnea, but who have failed multiple tube occlusion attempts or attempted extubation.
1) Electronic laryngoscopy reveals good mobility of both or at least one vocal cord, with laryngeal or tracheal
granulation tissue obstructing > 50% of the tracheal lumen, and normal mouth opening.
2) Electronic laryngoscopy indicates a penetration-aspiration score ≤ 4 points and a swallowing impairment assessment
score < 3 points.
3) Three-dimensional reconstruction of laryngotracheal CT shows soft tissue.
4) Obstruction above the tracheostomy site.
5) The patient or their family strongly requests extubation.
6) Other surgical contraindications are excluded.
All patients underwent endoscopic-assisted laryngotracheal granuloma resection under general anesthesia with suspension laryngoscopy. The procedures were successfully completed without complications. All patients achieved successful tube occlusion and decannulation within 7 to 10 days postoperatively.
Results
Causes of Laryngotracheal Stenosis in Patients with Long-Term Tracheostomy Tube Dependence After Brain Disease
Laryngotracheal Granulation Tissue Hyperplasia Obstructing the Trachea.
In this cohort of 27 patients, 26 cases (96.3%) were attributed to laryngotracheal granulation tissue hyperplasia obstructing the trachea, leading to extubation failure. All these patients achieved successful decannulation after surgical intervention.
Impaired Bilateral Vocal Cord Abduction.
Only 1 patient (3.7%) in the cohort experienced extubation failure due to bilateral vocal cord fixation with impaired abduction.
Endoscopic-Assisted Laryngotracheal Granuloma Resection Under General Anesthesia: A Safe and Effective Approach.
Endoscopic-assisted laryngotracheal granuloma resection under general anesthesia with suspension laryngoscopy proved to be a safe and effective method for resolving extubation difficulties in such patients. The procedures were completed successfully without complications.
Discussion
Impact of Long-Term Tracheostomy Tube Dependence on Patients' Quality of Life
Tracheostomy tubes significantly impair fundamental life functions, including respiration, swallowing, and nutritional intake. Prolonged tube retention can lead to excessive secretions or complications such as tracheal obstruction, exacerbating patient discomfort [1]. Multiple studies indicate a substantial decline in quality of life among patients with long-term tracheostomy tube dependence [2-3]. This phenomenon, described as "severely compromised quality of life," is particularly evident in patients with extended tube dependence (e.g. 3-12 months), showing a significant gap compared to non-tracheostomy patients [5]. The detrimental effects manifest across multiple dimensions, as summarized below:
Swallowing and Respiratory Functions
After tracheostomy tube placement, patients frequently experience dysphagia (reported in 44% of cases), dyspnea, pain, and restricted mobility [4]. Pediatric patients may face developmental delays and neurocognitive impairments [5]. In terms of respiratory mechanics, long-term tube dependence alters breathing function. For instance, tracheostomy reduces airway resistance, decreasing respiratory work but potentially leading to respiratory muscle atrophy due to disuse. In patients requiring prolonged mechanical ventilation, the tube's persistent presence can cause structural damage to the trachea, such as scar formation, tracheal stenosis, or malacia [6]. Complications like tube displacement or blockage may precipitate acute respiratory failure [7], while tube malposition or barotrauma can cause pneumomediastinum as air leaks into surrounding tissues, compressing the airway [8]. Studies also indicate weakened pharyngeal reflexes and increased gastroesophageal reflux (p < 0.05) in long-term tube-dependent patients, elevating aspiration risks and secondary pneumonia [9]. Difficult decannulation is common: one study found that although 57% of patients achieved short-term decannulation, 32% required reinsertion within two years due to respiratory issues, suggesting incomplete functional recovery. These factors contribute to sustained reliance on mechanical ventilation support [10].
Respiratory Infections
From a physiological perspective, tracheostomy alters the normal anatomy and function of the respiratory tract, compromising the warming, humidifying, and filtering capabilities of the upper airways. This allows inhaled air to directly enter the lower respiratory tract, leading to dryness of the airway mucosa and thickened secretions. Long-term tube retention can induce chronic inflammation in the respiratory tract, thereby increasing the risk of pulmonary infections. A retrospective cohort study demonstrated that among patients with severe traumatic brain injury, the incidence of pulmonary infections following tracheostomy reached as high as 26.85% [11]. Frequent respiratory infections not only cause physical discomfort but may also lead to increased hospitalizations and healthcare costs, further impairing patients' quality of life.
Impact of Long-Term Tracheostomy Tube Dependence on Patients' Psychological and Social Functioning
Long-term tracheostomy tube dependence frequently leads to psychological disturbances, including diminished self-esteem, anxiety, stress, and depression. Communication barriers—particularly the inability to speak normally— directly undermine self-image and social adaptability. Anxiety and depression are the most prevalent psychological issues in this population. A study of 89 patients recorded pre-intervention scores of SAS: 56.78 ± 6.42 and SDS: 57.62 ± 7.12, both significantly exceeding normal thresholds, indicating widespread moderate-to-severe anxiety and depressive symptoms. The visible tracheostomy tube on the neck acts as a social stigma, further inhibiting social interaction [12]. Due to the need for frequent stoma care, infection concerns, fear of negative social perceptions, and general functional decline, patients often progressively reduce social activities.
Impact of Long-Term Tracheostomy Tube Dependence on Family and Economic Burden
For patients with long-term tracheostomy tube dependence, the challenges extend beyond health issues to significant family and economic burdens. In addition to direct medical costs, prolonged tube retention often leads to reduced or complete loss of labor capacity, resulting in decreased household income. Simultaneously, caregivers may be forced to leave their jobs to provide full-time care, further exacerbating financial strain. The uncertainty of the patient's condition, potential complications (e.g., tube blockage or infection), and concerns about long-term quality of life contribute to chronic psychological stress among family members, manifesting as anxiety, depression, and emotional exhaustion. This psychological burden not only affects caregivers' well-being but may also indirectly hinder the patient's recovery process by compromising the quality of home care.
Reasons for Difficult Decannulation in Patients with Brain Diseases After Long-Term Tracheostomy
Laryngotracheal stenosis (LTS) is a major cause of decannulation failure. It can result from iatrogenic injury, trauma, infection, autoimmune diseases, or congenital anomalies, with prolonged endotracheal intubation or tracheostomy being the most common predisposing factors. Stenosis typically occurs in the subglottic region or cervical trachea, primarily due to abnormal mucosal repair and fibrosis following mechanical injury. In the present case series, granulation tissue hyperplasia obstructing the tracheal lumen was the leading cause of decannulation failure in 26 patients (96.3%), while only 1 case (6.7%) resulted from bilateral vocal fold immobility.
Clinical Management
1. Detailed history taking to assess whether the primary brain disease is stable and whether the patient or family
members have a strong desire for decannulation.
2. Preoperative electronic laryngoscopy to comprehensively evaluate swallowing function, including grading of
penetration and aspiration, secretions scale scoring, and documentation with photos and videos. Simultaneously,
laryngotracheal CT three-dimensional reconstruction is performed to quantify the degree of stenosis or
obstruction.
3. Strict adherence to indication criteria for surgical intervention. All patients underwent endoscopic-assisted
laryngotracheal granuloma resection under general anesthesia with suspension laryngoscopy. The procedures were
completed successfully without complications. Decannulation was achieved within 7-10 days postoperatively in all
cases.
Finally, due to the retrospective nature of this study, specific details regarding baseline airway management—such as precise tracheostomy tube sizes, cuff management protocols, and the exact duration of prior endotracheal intubation— were inconsistently documented in the historical medical records and could not be analyzed. Future prospective studies are warranted to evaluate the impact of these specific variables on decannulation outcomes.
Conclusion
In conclusion, electronic fiberoptic laryngoscopy and laryngotracheal CT three-dimensional reconstruction serve as reliable preoperative modalities for examination and evaluation. These complementary techniques enable precise selection of suitable surgical candidates. Furthermore, endoscopic-assisted resection of laryngotracheal granulation lesions via a supporting laryngoscope under general anesthesia is demonstrated to be a safe and effective approach for addressing decannulation difficulties in this patient population.
Abbreviations
ABI: Acquired Brain Injury; CT: Computed Tomography; FEES: Fiberoptic Endoscopic Evaluation of Swallowing; LTS: Laryngotracheal Stenosis; PAS: Penetration-Aspiration Scale; QOL: Quality of Life; SAS: Self-Rating Anxiety Scale; SDS: Self-Rating Depression Scale; SpO2: Resting Blood Oxygen Saturation; WHO-QOL BREF: World Health Organization Quality of Life BREF Questionnaire.
Declarations
Acknowledgements
We would like to thank the anonymous reviewers and the editors for their constructive comments.
Author Contributions
Haiwen Hu designed the study, performed the experiments and data analysis. Quanhui Guo wrote the manuscript. All authors read and approved the final manuscript. The author(s) report no conflicts of interest in this work.
Funding information
This research received no external funding.
Ethics Approval and Consent to Participate
Not applicable.
Competing Interests
The authors declare no competing interests.
Data availability
All data generated or analyzed during this study are included in this published article.
References
 Figures
Figures References
References Peer
Peer Information
InformationFigure 1. Laryngotracheal CT Image.
Figure 2. Preoperative images of laryngoscopy.
Figure 3. Postoperative images of laryngoscopy.
Peer-review Terminology
Identity transparency: Single anonymized
Reviewer interacts with: Editor
Details
This is an open access article under the terms of the Creative Commons Attribution License(http://creativecommons.org/licenses/by/4.0/), which permits use, distribution and reproduction in any medium, provided the original work is properly cited.
Publication History
Received 2026-01-22
Accepted 2026-03-25
Published 2026-04-03