




Abstract
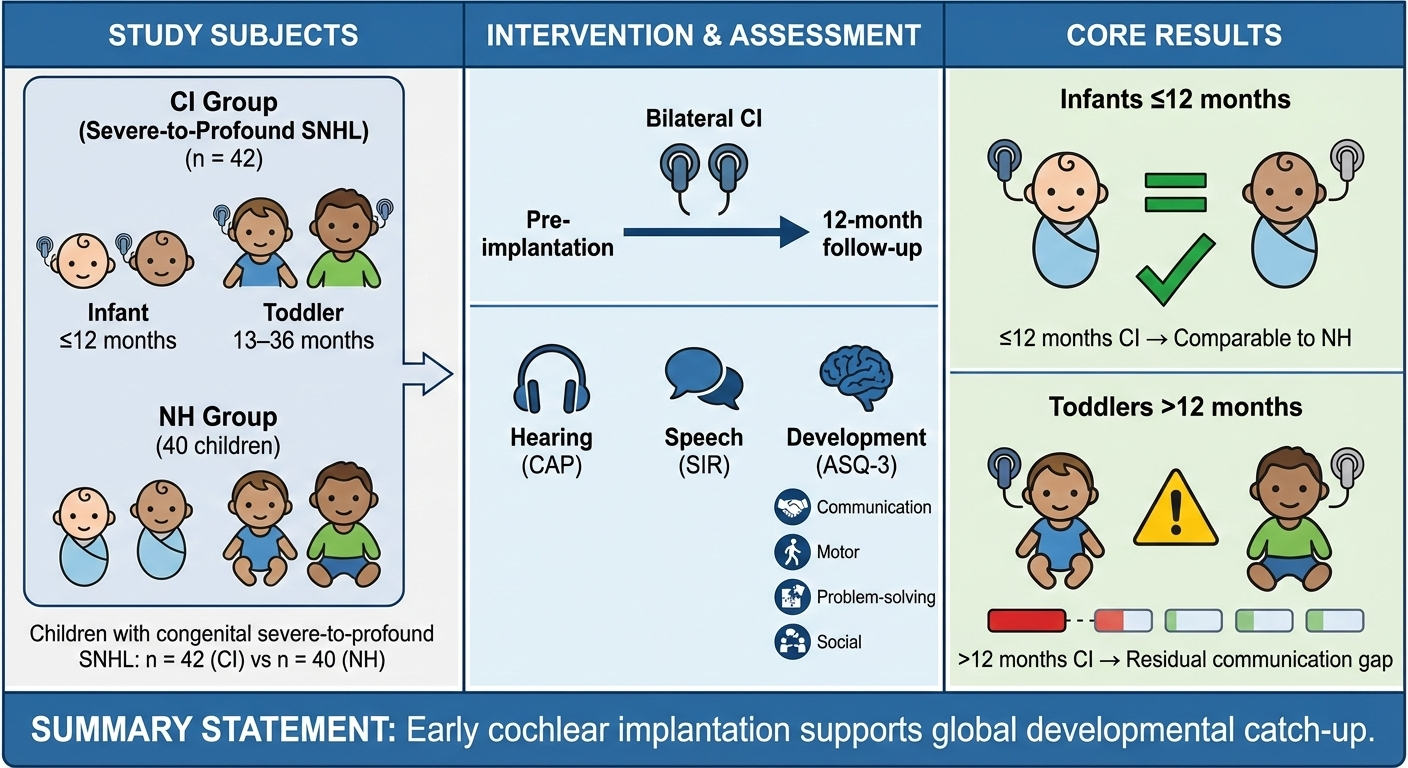
Objective: To evaluate whether early cochlear implant (CI) use can significantly and positively change hearing and speech abilities during a child's development.
Methods: The present study included 42 children with bilateral CIs (8–36 months) and 40 age-matched children with normal hearing (NH) (6–48 months). Ages & Stages Questionnaires, Third Edition (ASQ-3); Categories of Auditory Performance (CAP); Speech Intelligibility Rate (SIR) were used.
Results: Twelve months after receiving bilateral CIs, the hearing status of the infants (1–12 months) and toddlers (13–36 months) had improved significantly. Infants using CIs were comparable to those with NH in all ASQ-3 aspects (p > 0.05). For toddlers, there was a post-implantation improvement in the gross motor, problem solving, and personal-social domains (p > 0.05). However, there were still gaps in the communication domain (p < 0.001). Multivariate analysis revealed that pre-implantation hearing aid usage duration, schooling, SIR score, communication, and caregiver education level significantly influenced post-implantation outcomes.
Conclusions: With CI use, infants and toddlers with congenital sensorineural hearing loss showed improvements in auditory perception, speech production, and developmental abilities. Infant implant recipients performed better in all areas of development than toddlers, comparable to NH children. Hearing aid use, language rehabilitation training, caregivers' education level, and communication method were all highly correlated with the overall development of the children.
Keywords: Cochlear implants; Development; Auditory; Speech.
Introduction
Hearing loss is a growing global health challenge affecting individuals across the lifespan. Recent data from the Global Burden of Disease Study highlights the increasing prevalence of hearing loss, emphasizing the need for early intervention strategies [1-3]. Hearing allows children to sense the world around them, communicate with others, acquire knowledge, and integrate into society. Auditory deprivation from birth notably hampers a child's development. Fortunately, cochlear implant (CI) use can reduce the consequences of auditory deprivation, showing how far biomedical science has progressed.
Cochlear implantation has proved to be a safe and effective treatment for children with severe-to-profound sensorineural hearing loss. CI use can help restore auditory and speech functions to varying degrees [4]. The timing of implantation is critical. Multiple lines of evidence suggest that infants who undergo implantation before 12 months exhibit better auditory performance and speech outcomes than children implanted after 12 months [5-7]. It is highly probable that the reason for this is the time-sensitive window during which the auditory cortex matures, a period when the central auditory pathways exhibit maximum plasticity [8-10]. This window spans a child's first 48 months of life.
Monitoring the effects of CI use mainly focuses on tangible aspects of hearing and speech capabilities. However, cognitive development dimensions that are less directly associated with hearing are yet to be investigated [11]. The child's overall developmental status is a potential predictor of cognitive function after receiving a CI [34]. Monitoring cognitive development dimensions should be valued with equal, if not more, importance to traditional measures. The rationale lies in the fact that brain development happens in a systematic manner [12]. Hearing loss can have knock-on effects on other functions, including higher-order neurocognitive tasks [13]. It has been found that early deafness will hamper a child's overall development, including cognitive, motor, and social domains [14-18]. This has also been acknowledged by national guidelines for early screening; children's hearing problems should be addressed as early as possible to prevent possible developmental delays, allowing them to reach their full potential [19-22].
The present study aims to find out whether early implantation can significantly improve a child's overall development, as well as hearing and speech abilities.
Materials and methods
ParticipantsThe present retrospective study focused on infants (aged 1–12 months) and toddlers (aged 13–36 months) who had received bilateral CIs at the ENT department of the Second Affiliated Hospital of Anhui Medical University between 2019 and 2021. All the CI recipients were born with severe-to-profound hearing loss, while the control group consisted of children with normal hearing.
Data from the CI recipients were primarily collected in offline forms. The data included details such as age, gender, inner ear anomalies, cerebral lesions, hearing aid use, caregiver's education level, post-implantation communication mode (Communication modes were categorized into oral and multiple types. The 'multiple communication type' was defined as the simultaneous use of speech and sign language or a combination of oral communication with gestures.), and aural rehabilitation (Table 1). Consent was received from all the participants' parents prior to filling out the questionnaire, as well as basic information for the NH children. On top of this, the study protocol was reviewed and approved by our hospital's ethics committee.
From the preoperative brain magnetic resonance imaging (MRI) and high-resolution computed tomography (HRCT), the inner ear anomalies included enlarged vestibular aqueduct (n=5), incomplete partition II (n=7), internal auditory canal stenosis (n=4), and focal parenchymal lesion (n=4). Some cases included more than one inner ear anomaly. It was noted that all the children had no congenital diseases except hearing loss before surgery. All the patients had the same doctor performing the surgery and an artificial cochlea of the same brand. The system was activated normally one month after surgery. The data were recorded 1 day before and 12 months after the surgery.
The control group included 40 children distributed across the age spectrum to match the CI cohort. Gender distribution in the NH group (21 boys and 19 girls) was not significantly different from the CI group (p > 0.05). Specifically, this included 11 children aged under 12 months, 11 children aged 13–24 months, 6 children aged 25–36 months and 12 children aged 36–48 months. Their ASQ-3 scores were within the normal range.
A total of 42 children with bilateral CIs and 40 children with normal hearing were initially screened. The detailed inclusion and exclusion process, as well as the final cohort composition, is illustrated in the study flowchart (Figure 1).
Figure 1. This flowchart illustrates the screening and enrollment process for children in the study. The pathway details the inclusion of children with congenital severe-to-profound sensorineural hearing loss (CI group, n = 42), stratified by age at implantation (≤12 months and >12 months). The right pathway shows the enrollment of age-matched children with normal hearing (NH group, n = 40). Excluded participants and reasons are specified. All CI recipients underwent a 12-month post-implantation assessment using the ASQ-3, and their outcomes were compared with those of the NH group. Key influencing factors analyzed included pre-implantation hearing aid use, communication mode, schooling status, aural rehabilitation, caregiver education level, CAP, and SIR scores.
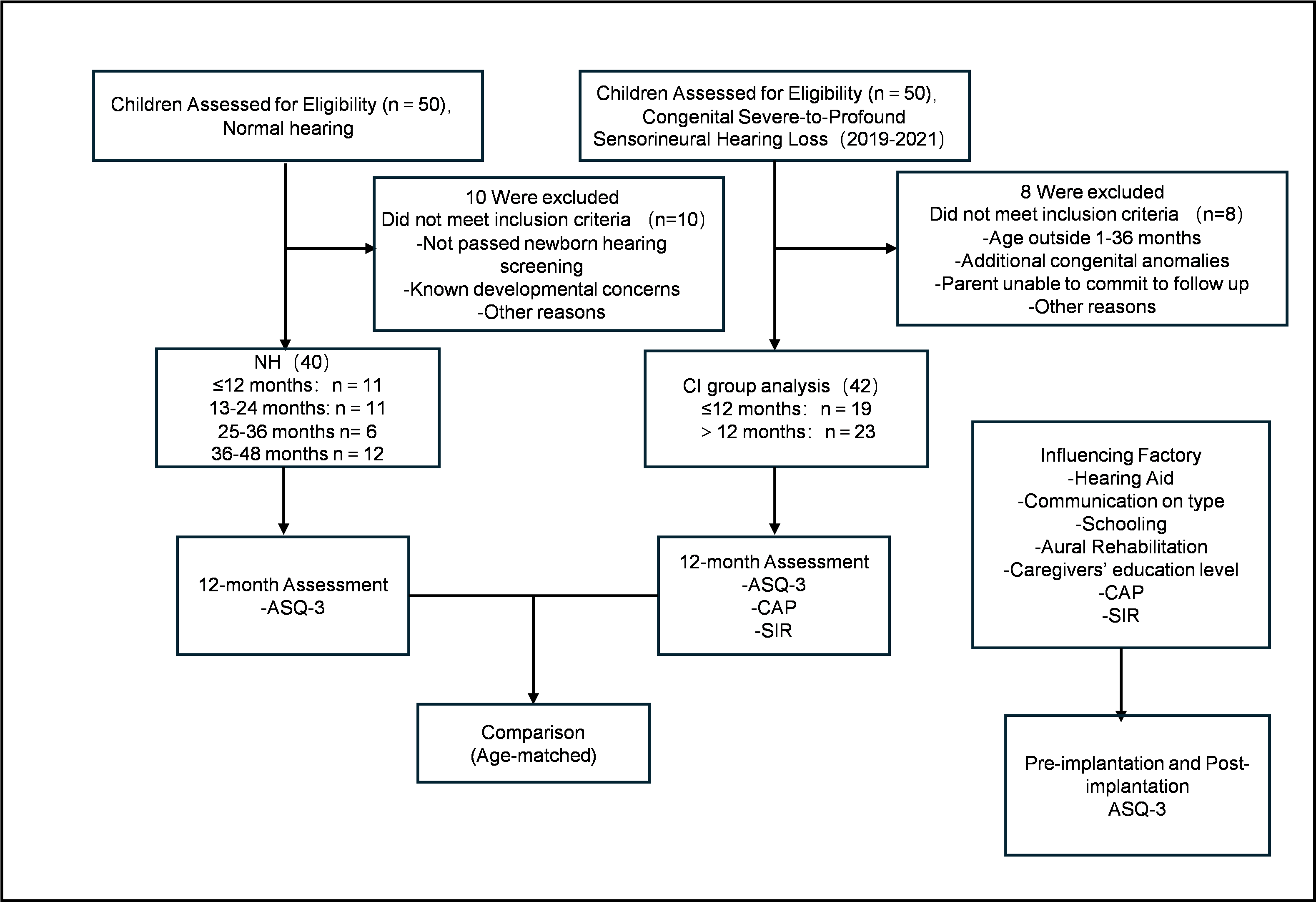
Table 1. Demographic characteristics of CI recipients.
| Characteristic | Category | CI recipients (≤ 12 months) | CI recipients (12-36 months) |
|---|---|---|---|
| Age (months) | Mean ± SD | 9.37±1.51 | 26.22±5.56 |
| Sex | Female | 6 | 13 |
| Male | 13 | 10 | |
| Inner ear anomalies | None | 12 | 12 |
| Anomalies | 7 | 11 | |
| Cerebral lesions | None | 18 | 23 |
| Anomalies | 1 | 0 | |
| Hearing aids | Yes | 11 | 10 |
| No | 8 | 13 | |
| Caregiver's education level | None | 1 | 0 |
| Primary school | 1 | 3 | |
| Junior high school | 8 | 8 | |
| Senior high school | 5 | 2 | |
| University degree | 4 | 10 | |
| Communication mode | Oral | 19 | 21 |
| Sign language + Oral | 0 | 2 | |
| Aural rehabilitation | No | 3 | 0 |
| Yes | 16 | 23 | |
| Schooling status | No school | 9 | 0 |
| Kindergarten | 10 | 9 | |
| Rehabilitation school | 0 | 14 |
Auditory and speech evaluation
Categories of Auditory Performance (CAP) is a scale used to assess the post-implantation auditory perception abilities of children who have received CIs. CAP provides 8 categories to rate hearing abilities, in order of increasing ability (Table S1) [23-24].
The Speech Intelligibility Rating (SIR) scale is used to assess the speech intelligibility of children who have received CIs. It provides 5 categories for evaluating spontaneous speech (Table S2) [25].
Development evaluation
The Ages & Stages Questionnaires, Third Version (ASQ-3) is an instrument completed by parents/caregivers to identify developmental delays in children aged 2–66 months [26]. It consists of 21 questionnaires for different age ranges. Each questionnaire consists of 30 items divided into 5 dimensions: 1) communication, 2) gross motor, 3) fine motor, 4) problem solving, and 5) personal-social.
The ASQ-3 has been translated into several languages, including Chinese [24]. It has excellent psychometric properties, with a test–retest reliability of 92%, a sensitivity of 87.4%, and a specificity of 95.7%, which has been tested worldwide [27–30].
The ASQ-3's easy-to-understand questions are filled out by the primary caregiver, such as the parent. Based on each section's score, the assessor determines whether the child's development is consistent with their age level, effectively identifying possible developmental delays.
Statistical AnalysisSPSS software version 26.0 was used for the data analysis. First, descriptive statistics were used to summarize the variables and calculate the frequencies and percentages of numeric variables. The Shapiro–Wilk test was used to verify the normality of numeric variables (p < 0.05). Due to the non-normal distribution of the data, the Wilcoxon signed-rank test was subsequently used to compare pre- and post-surgery paired scores. The Mann–Whitney U test was then used to compare overall differences between children with CIs and NH children.
Additionally, multivariate linear regression analysis was used to explore the combined effects of multiple independent variables on the baseline scores across the 5 ASQ-3 subscales before the surgery. Generalized linear regression analysis was also used to identify the factors influencing the post-implantation improvement in the five ASQ-3 subscales. All significance tests were set at a 95% confidence interval and a significance level of 0.05.
Results
Pre- and post-implantation comparison among children with CIsTable 2 shows the Wilcoxon signed-rank test results for the ASQ-3, CAP, and SIR for CI children pre- and 12 months post-implantation. The results indicated significant improvement after CI use in the communication (p < 0.01), gross motor, problem solving (p < 0.01), and personal-social domains, as well as CAP (p < 0.01) and SIR (p < 0.01) scores. However, the fine motor domain did not show a significant improvement. CI use proved to have a significant positive effect on overall development level, auditory performance, and speech intelligibility.
Table 2. Wilcoxon signed-rank test results comparing pre- and post-implantation ASQ-3, CAP, and SIR scores for children with CIs.
| Instrument | Domain / Subscale | z-value | p-value |
|---|---|---|---|
| ASQ-3 | Communication | 3.83237 | <.001 |
| Gross motor | -2.78832 | 0.006 | |
| Fine motor | -1.45668 | 0.981 | |
| Problem-solving | 3.82612 | <.001 | |
| Personal-social | 1.42542 | 0.035 | |
| CAP | - | 52.04805 | <.001 |
| SIR | - | 52.04805 | <.001 |
Figure 2 and Table 3 show the significant differences in ASQ-3 scores between children with CIs and NH children pre- and 12 months post-implantation. The performance of children with CIs was below that of NH children. Before surgery, all ASQ-3 domains except for fine motor had significant differences (p < 0.01). After surgery, there was a noticeable improvement in the gross motor, fine motor, and personal-social domains, and the mean gap had narrowed in others, indicating the positive impact of CI use.
Figure 2. Comparison of developmental outcomes before and after cochlear implantation. (a) (Left panel): Bar graph comparing ASQ-3 domain scores (communication, gross motor, fine motor, problem-solving, personal-social) in children with CIs before (CI Pre) and 12 months after (CI Post) implantation. Error bars represent standard deviations. Asterisks denote statistically significant improvements post-implantation (**p < 0.01, *p < 0.05). (b) (Right panel): Bar graph comparing ASQ-3 domain scores between children with CIs 12 months post-implantation (CI Post) and age-matched children with normal hearing (NH). The dashed line represents the NH group's mean score level for reference. Gaps, particularly in the communication domain, are evident between the CI Post and NH groups.
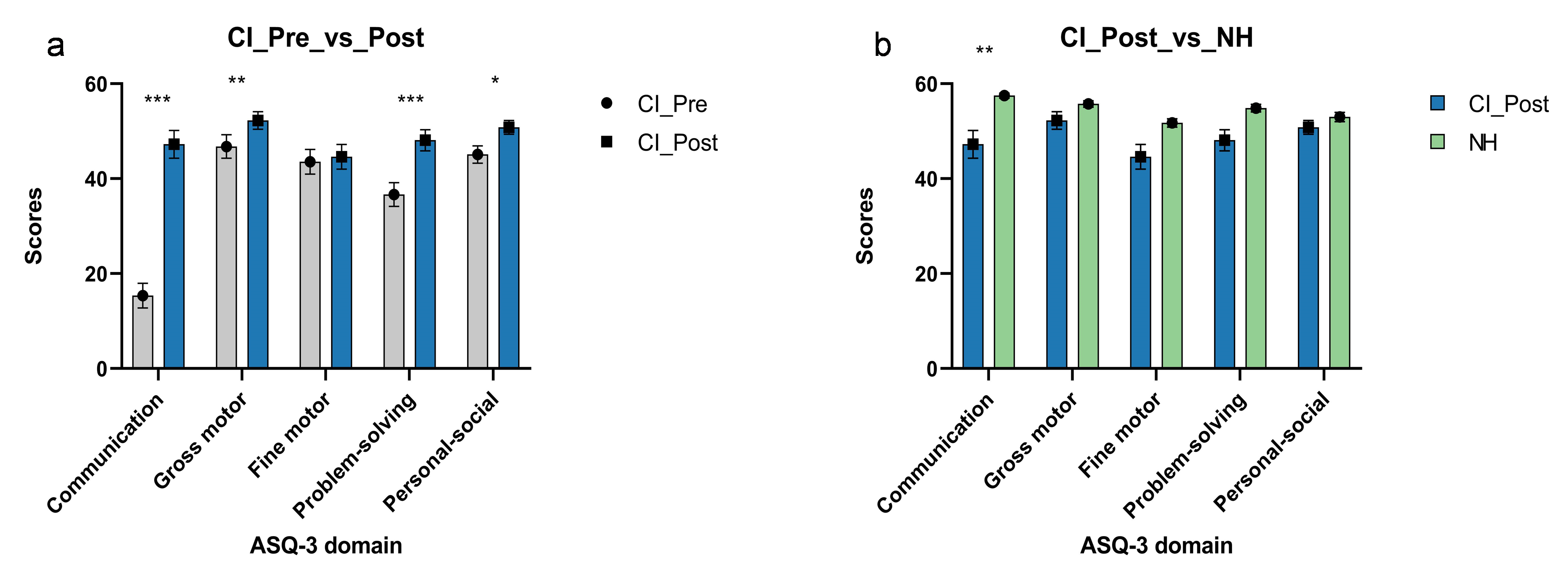
Table 3. Mann–Whitney U test results comparing pre- and post-implantation ASQ-3 scores between children with CIs and NH children.
| ASQ-3 domain | Time point | CI recipients (n = 42) | NH (n = 40) | p-value |
|---|---|---|---|---|
| Communication | Pre-implantation | 15.36± 2.61 | 57.5 ± 0.54 | <0.001 |
| Post-implantation | 47.26 ± 2.91 | 57.5 ± 0.54 | 0.004 | |
| Gross motor | Pre-implantation | 46.79 ± 2.48 | 55.75 ± 0.68 | 0.011 |
| Post-implantation | 52.26 ± 1.84 | 55.75 ± 0.68 | 0.788 | |
| Fine motor | Pre-implantation | 43.57 ± 2.62 | 51.75 ± 0.89 | 0.174 |
| Post-implantation | 44.64 ± 2.60 | 51.75 ± 0.89 | 0.339 | |
| Problem-solving | Pre-implantation | 36.67 ± 2.50 | 54.88 ± 0.79 | <0.001 |
| Post-implantation | 48.10 ± 2.20 | 54.88 ± 0.79 | 0.085 | |
| Personal-social | Pre-implantation | 45.12 ± 1.83 | 53.00 ± 0.96 | 0.004 |
| Post-implantation | 50.83 ± 1.46 | 53.00 ± 0.96 | 0.519 |
Figure 3 and Table S3 show the Mann–Whitney U test results for the ASQ-3 scores of the 19 children with CIs and the 11 NH children aged ≤ 12 months. Before implantation, there was no significant difference between the two groups' fine motor domains, but the other domains were significantly different (p < 0.05). The scores of the children with CIs were comparable to those of the 11 NH children at the same follow-up age in all domains 24 months post-implantation (p > 0.05).
Figure 3 and Table S3 also show the Mann–Whitney U test results for children ≥ 12 months. Before implantation, comparisons between children with deafness and NH children showed statistically significant differences in the communication (p < 0.01) and problem solving (p < 0.01) domains. When comparing children with CIs aged ≥ 12 months with NH children aged 24–48 months, there was an improvement in the gross motor, problem solving, and personal-social domains 12 months post-implantation (p > 0.05). However, there were still gaps in the communication domain (p < 0.01). The general positive effects of CI use were better in children ≤ 12 months than in children ≥ 12 months. This implies that the timing of surgical intervention is critical. In terms of the communication, fine motor, and personal-social domains, the scores decreased with age. The data demonstrate that the positive effects of CI use decrease as the recipient's age at implantation increases.
Figure 3. Developmental outcomes stratified by age at implantation. (a) (Upper panel): Comparison of ASQ-3 scores between infants who received CIs at ≤ 12 months of age (CI Infants) and age-matched infants with normal hearing (NH Infants) at the 12-month follow-up. Infants with CIs achieved scores comparable to their NH peers across all developmental domains. (b) (Lower panel): Comparison of ASQ-3 scores between toddlers who received CIs at > 12 months of age (CI Toddlers) and age-matched toddlers with normal hearing (NH Toddlers). While improvements were observed in gross motor, problem-solving, and personal-social domains, a significant gap remained in the communication domain for the CI Toddlers group.
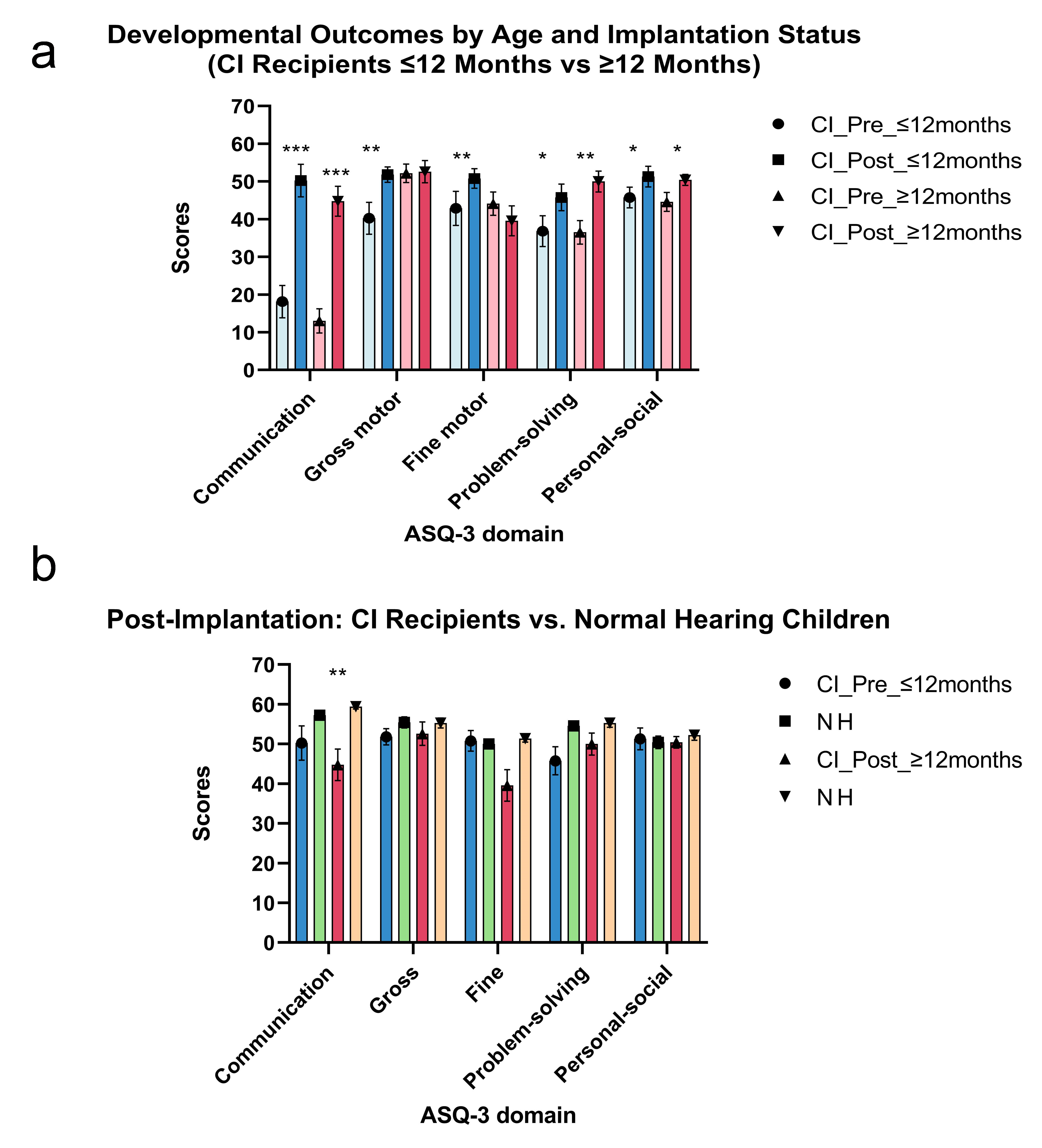
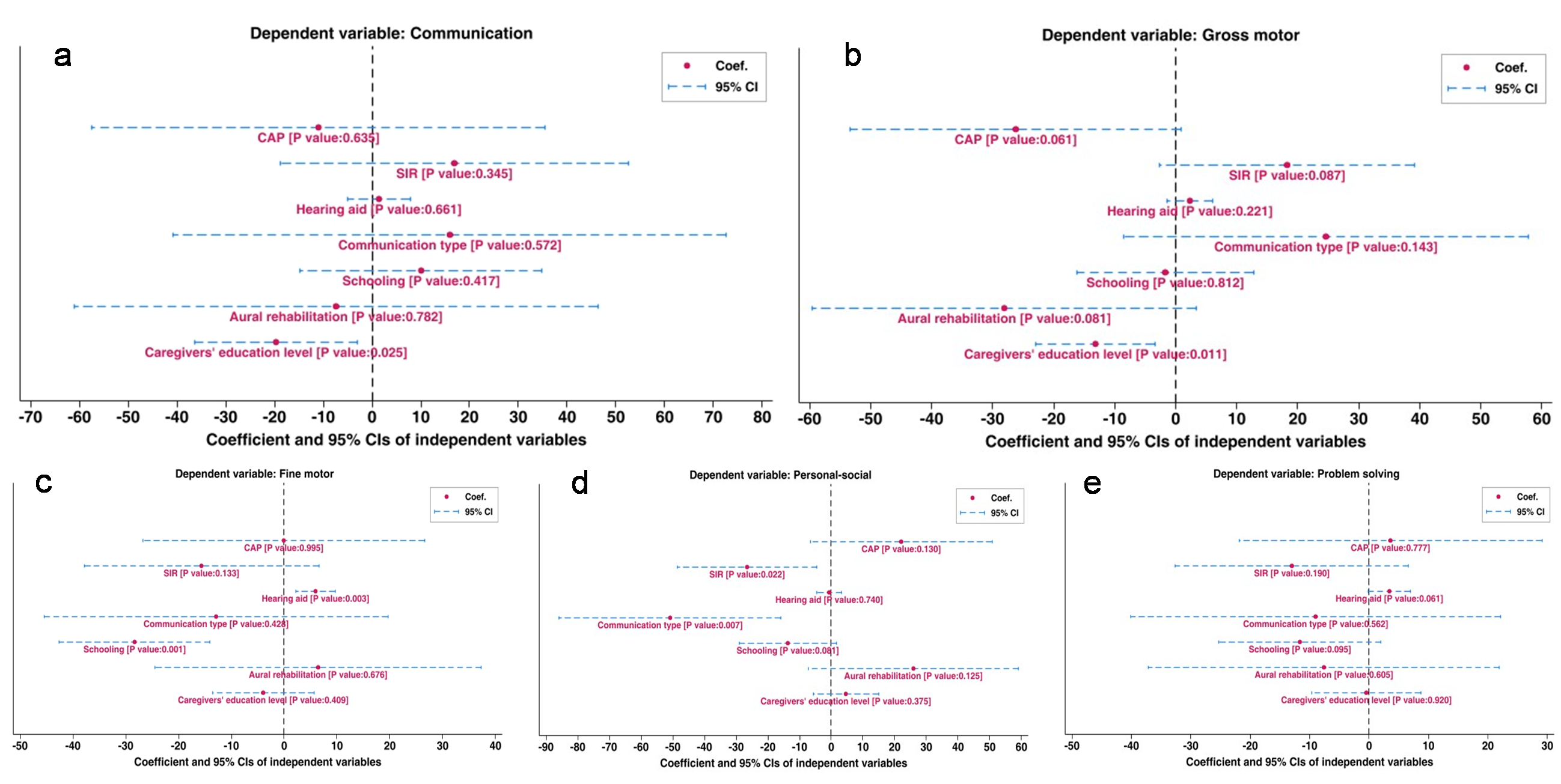
Figure 4 shows the generalized linear regression analysis results examining the factors influencing the post-implantation improvement in the 5 ASQ-3 domains in children with CIs. The predictors analyzed consist of CAP, SIR, hearing aid, communication type, schooling, aural rehabilitation, and caregivers' education level and individual difference.
Caregivers' education level significantly negatively affected post-implantation communication improvement, indicating that higher caregiver education levels were associated with smaller communication improvements. Pre-implantation hearing aid usage time and schooling status (p < .001) significantly influenced post-implantation fine motor improvement. Longer hearing aid usage was associated with greater improvement in the fine motor domain. Children without schooling showed larger improvements in the fine motor domain. The subject also significantly affected the results, highlighting variability in post-implantation improvements among children. Multiple communication types had a significant negative impact on post-implantation personal-social improvement, suggesting that certain communication modes (e.g., non-verbal communication) may hinder the development of social skills. Lower SIR scores also negatively affected social improvement, indicating that children with poorer speech understanding showed smaller gains in social abilities. The detailed results can be found in Table S4.
Figure 4. Factors influencing post-implantation developmental improvement. Results of the generalized linear regression analysis identifying predictors of improvement in the five ASQ-3 domains 12 months after cochlear implantation. The forest plot displays estimated coefficients (β) with 95% confidence intervals for each factor: pre-implantation hearing aid use duration, communication mode (oral vs. mixed), schooling status, aural rehabilitation attendance, caregiver education level, Categories of Auditory Performance (CAP) score, and Speech Intelligibility Rating (SIR) score. Factors with confidence intervals not crossing the zero line (vertical dashed line) are considered statistically significant predictors (p < 0.05).
Discussion
With the development of science and technology, biomedical technology has made great progress. This includes cochlear, vestibular, and retinal implants, among which cochlear implantation enjoys great success [17]. Because the human cochlea begins to function between 24 and 36 weeks of gestational age, the effects on hearing may begin during intrauterine life [31], which is earlier than previously thought. Also, early deafness is often considered a connectome disease that affects the central nervous system [17], blocking the transmission of information from peripheral hearing to higher auditory centers, and affecting the interconnections between the centers and multiple cortical areas. Therefore, due to the influence of multiple factors, children will not only show different improvements in hearing and speech after CI use but may also have differences in development.
Our study showed that CI use led to improvements in auditory and speech intelligibility abilities in children with severe-to-profound deafness 12 months post-implantation. The use of CAP and SIR helped us to quickly assess each child's condition, offering the advantage of early detection and intervention for children of all ages. All children underwent bilateral cochlear implantation, which was consistent with previous evidence [33] that early bilateral cochlear implantation can significantly improve children's auditory and speech intelligibility prognoses.
As more and more children are implanted bilaterally, the post-implantation areas of focus have become more comprehensive. Previous research has found that a child's overall development status is a potential predictor of cognitive function after CI use [34]. However, it is difficult to assess the cognitive function of infants and toddlers directly, particularly when they have profound sensorineural hearing loss. This is due to them being unable to conduct the tests themselves and communicate effectively. Therefore, assessing the child's overall development status can help us solve this problem and figure out the child's cognitive status. Depending on the purpose of the test, the scales can be divided into diagnostic scales and screening scales. Although diagnostic scales are relatively accurate, they are complex and time-consuming, (e.g., the Gesell Developmental Diagnosis Scale [35] and the Bayley Scales for Infant Development, Third Edition [36]). The screening scales are simple to operate and have low medical costs, making them more suitable for regular screening and monitoring for early detection, early diagnosis, and early intervention, (e.g., the Denver Developmental Screening Test [37] and the ASQ-3 [26]).
The ASQ-3 can help to find out whether children aged 2–66 months have developmental delays [26]. It is one of the most widely used screening assessments of early childhood. Previous data from animal models and children with deafness have shown that there is a sensitive period for the maturation of the auditory cortex in the first 48 months of life [38]. CI use can alleviate auditory system deficits and promote cortical maturation in children with deafness [39]. Restoring hearing during this period can both stimulate the development of cortical function to a great extent and provide conditions in which auditory speech abilities and overall development can improve. The ASQ-3's target age group roughly coincides with the cortex's sensitive period, which covers the years from infancy to toddlerhood. The ASQ-3 can evaluate infants' and toddlers' overall developmental levels to timely discover low-level development situations, carry out appropriate interventions, reduce the risks of such diseases, and improve the population's quality of life.
Current literature shows that children with CIs experience difficulties with fine and gross motor skills, social interaction, and cognitive abilities [40]. Conversely, our study demonstrated that CI use led to children making significant progress in the communication, gross motor, problem solving, and personal-social domains. However, a notable exception was observed in the fine motor domain, where no significant 'catch-up' occurred relative to NH peers. This specific lag warrants explanation beyond general developmental delay and is likely attributable to complex physiological constraints. Recent evidence suggests that fine motor deficits in this population are closely linked to vestibular dysfunction, which is highly prevalent (up to 60%) in children with sensorineural hearing loss [41]. The vestibular system is critical not merely for balance, but for maintaining the proximal stability and postural tone required for precise distal movements; thus, compromised vestibular input can impede the maturation of fine finger dexterity even after auditory restoration [42]. Except for the fine motor domain, children with hearing loss fall behind NH children in all other domains. Auditory deprivation in infants leads to a significant decline in fine motor function as they age [43]. Our findings suggest that CI use alleviates this downward trend: just 12 months after cochlear implantation, children with deafness showed significant improvements in gross and fine motor, problem solving, and personal-social domains, and the communication gap between children with CIs and NH children also narrowed.
Research related to the development of children with congenital deafness shows that infants who received CIs before 12 months developed better in terms of hearing and speech than those implanted after, and even reached the standards of NH children [6, 44, 45]. At the same time, no significant age-related surgical complications have been reported [7, 46]. Therefore, we divided the children into two age groups: infants ≤ 12 months and toddlers ≥ 12 months. We found that, with bilateral CI use, infants with hearing loss achieve almost the same development level as NH children. However, toddlers still had communication gaps. These results indicate that CI use could help children with hearing loss develop, but this effect may decline with age. Multiple research reports showed that cochlear implantation at ≤ 12 months of age had significant advantages in long-term post-implantation language skills and cognitive development outcomes [47-48]. Therefore, to allow children with deafness to develop at a better rate, we recommend that bilateral CI surgery should be performed before 12 months, if possible.
The present study found that higher levels of caregiver education are associated with poorer post-implantation communication skills in children with deafness. Previous studies have shown that parents' high level of education can improve children's developmental delays [49-50], which contradicts our research. We theorize that this may be due to caregivers with higher education levels having elevated expectations for the communication skills of their children with deafness, leading to a decrease in scores and thus affecting the ASQ-3 score. Gross motor skills involve the use of large muscle groups, while fine motor skills involve the use of smaller muscles / muscle groups. Together, they constitute components of human behavior with practical significance for day-to-day functioning [51]. Our research found a significant negative correlation between the educational level of caregivers and gross motor skills in children with deafness. We theorize that this may be because of the small sample size, which may not completely represent the entire population.
The present study found that wearing hearing aids pre-implantation has a significant positive effect on the post-implantation fine motor skills of children with deafness. This is consistent with several studies [52-54]. Other studies have also shown that exercise and language development are closely related [55, 56]. Early adoption of hearing aids exposes children with deafness to verbal language at an earlier age, enabling them to adapt more quickly after implantation. This is undoubtedly beneficial for the development of motor skills in children with deafness. Additionally, there is also a significant correlation between postoperative school attendance and individual differences in fine motor skills. We found that personal-social skills correlate significantly with speech intelligibility and communication type. According to current literature, the communication style and clarity of speech of CI users affect how others understand them, which in turn affects their social functioning [57]. Using SIR to evaluate the intelligibility of children with deafness can help predict their social skills and thus plan corresponding intervention strategies.
Additionally, compared to sign language, verbal communication is more conducive to the social skills of children with deafness. This also indirectly is confirmed by the reciprocal relationship between communication and overall development, which gives us great confidence that, with CI use, infants with prelingual deafness could reach outcomes comparable to NH children in the future. Moving forward, children who receive CIs early in life should be managed in a more holistic manner to improve language skills and overall development. It seems more important than ever to individually tailor interventions to each child, to help them reach their full potential.
Clinically, integrating ASQ-3 into routine post-implantation assessments can facilitate early identification of developmental delays, enabling such tailored interventions. To maximize effectiveness in the rehabilitation plan, priority should be given to wearing hearing aids before surgery, maintaining good communication, and providing high-quality rehabilitation training (e.g., rehabilitation schools).
Despite the results mentioned above, several limitations should be mentioned. Our study was retrospective in design, which limited the availability of participants' information. Furthermore, the sample size was relatively small and the follow-up time relatively short, which may have limited the robustness of our analysis. However, data collection is still ongoing, and future analyses will benefit from an increased sample size.
Conclusion
Early cochlear implantation (≤ 12 months) significantly enhances auditory, speech, and developmental outcomes in children with congenital sensorineural hearing loss, enabling them to match NH peers in developmental milestones. Hearing aid use, language rehabilitation training, caregivers' education levels, and communication method are all highly correlated with a child's overall development. Therefore, a comprehensive evaluation of a child's overall development level using the ASQ-3 could be useful to improve the post-implantation outcomes. These findings advocate for bilateral implantation, coupled with holistic, family-centered support, to optimize developmental trajectories in children aged ≤ 12 months with severe-to-profound sensorineural hearing loss.
Abbreviations
CI - Cochlear Implant; NH - Normal Hearing; ASQ-3 - Ages & Stages Questionnaires, Third Edition; CAP - Categories of Audi-tory Performance; SIR - Speech Intelligibility Rating.
Declarations
Acknowledgements
We sincerely thank the Natural Science Foundation of Anhui Province and the National Natural Science Foundation of China Incubation Program for their financial support of this research. We also extend our gratitude to the Department of Otorhinolaryngology, Head and Neck Surgery at The Second Affiliated Hospital of Anhui Medical University for providing the clinical data and research platform. We are particularly indebted to Dr. Wei Cao for his invaluable guidance throughout the study design and manuscript preparation. Additionally, we appreciate the statistical advice provided by our colleagues and the support from all the participating children and their families.
Author Contributions
Baodong Wu: Writing – original draft, Methodology, Investigation, Data curation, Formal analysis, Conceptualization. Yi Sun: Writing – review & editing, Project administration, Methodology, Data curation. Melcol Hailu Yilala: Writing – review, Supervision. Wei Cao: Writing – review & editing, Funding acquisition, Conceptualization.
Funding information
This research received funding from the Natural Science Foundation project of Anhui province [No. 2208085MH233] and the National Natural Science Foundation of China Incubation program [No. 2022GMFY03].
Ethics Approval and Consent to Participate
The study was conducted under the Declaration of Helsinki and approved by the Ethical Committee of the Second Affiliated Hospital of Anhui Medical University, Anhui, China. Informed consent was obtained from all subjects involved in the study.
Competing Interests
The authors declare no conflict of interest.
Data availability
The data presented in this study are available on request from the corresponding author.
References
 Figures
Figures References
References Peer
Peer Information
InformationFigure 1. This flowchart illustrates the screening and enrollment process for children in the study. The pathway details the inclusion of children with congenital severe-to-profound sensorineural hearing loss (CI group, n = 42), stratified by age at implantation (≤12 months and >12 months). The right pathway shows the enrollment of age-matched children with normal hearing (NH group, n = 40). Excluded participants and reasons are specified. All CI recipients underwent a 12-month post-implantation assessment using the ASQ-3, and their outcomes were compared with those of the NH group. Key influencing factors analyzed included pre-implantation hearing aid use, communication mode, schooling status, aural rehabilitation, caregiver education level, CAP, and SIR scores.
Figure 2. Comparison of developmental outcomes before and after cochlear implantation. (a) (Left panel): Bar graph comparing ASQ-3 domain scores (communication, gross motor, fine motor, problem-solving, personal-social) in children with CIs before (CI Pre) and 12 months after (CI Post) implantation. Error bars represent standard deviations. Asterisks denote statistically significant improvements post-implantation (**p < 0.01, *p < 0.05). (b) (Right panel): Bar graph comparing ASQ-3 domain scores between children with CIs 12 months post-implantation (CI Post) and age-matched children with normal hearing (NH). The dashed line represents the NH group's mean score level for reference. Gaps, particularly in the communication domain, are evident between the CI Post and NH groups.
Figure 3. Developmental outcomes stratified by age at implantation. (a) (Upper panel): Comparison of ASQ-3 scores between infants who received CIs at ≤ 12 months of age (CI Infants) and age-matched infants with normal hearing (NH Infants) at the 12-month follow-up. Infants with CIs achieved scores comparable to their NH peers across all developmental domains. (b) (Lower panel): Comparison of ASQ-3 scores between toddlers who received CIs at > 12 months of age (CI Toddlers) and age-matched toddlers with normal hearing (NH Toddlers). While improvements were observed in gross motor, problem-solving, and personal-social domains, a significant gap remained in the communication domain for the CI Toddlers group.
Figure 4. Factors influencing post-implantation developmental improvement. Results of the generalized linear regression analysis identifying predictors of improvement in the five ASQ-3 domains 12 months after cochlear implantation. The forest plot displays estimated coefficients (β) with 95% confidence intervals for each factor: pre-implantation hearing aid use duration, communication mode (oral vs. mixed), schooling status, aural rehabilitation attendance, caregiver education level, Categories of Auditory Performance (CAP) score, and Speech Intelligibility Rating (SIR) score. Factors with confidence intervals not crossing the zero line (vertical dashed line) are considered statistically significant predictors (p < 0.05).
[4]NIH Consensus Conference. Cochlear implants in adults and children. JAMA. 1995;274(24):1955–1961.
[35]Bayley N. Bayley Scales of Infant and Toddler Development Administration Manual. Pearson. 2006.
[50]Nagel M, Sharman R. The Encyclopedia of Child and Adolescent Development. Wiley. 2019.
Peer-review Terminology
Identity transparency: Single anonymized
Reviewer interacts with: Editor
Details
This is an open access article under the terms of the Creative Commons Attribution License(http://creativecommons.org/licenses/by/4.0/), which permits use, distribution and reproduction in any medium, provided the original work is properly cited.
Publication History
Received 2026-01-12
Accepted 2026-02-09
Published 2026-03-12